You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- TALBERT - 2012 - Inverted ClassroomDocument4 pagesTALBERT - 2012 - Inverted ClassroomMaribel Melissa Blas CadilloNo ratings yet
- Letter of Rec - Keller SibertDocument1 pageLetter of Rec - Keller Sibertapi-458156572No ratings yet
- ResumeDocument4 pagesResumeCheranmadevi PadavettanNo ratings yet
- Financial Planning Course Outline (Hanoi UniversityDocument5 pagesFinancial Planning Course Outline (Hanoi UniversityHiền NguyễnNo ratings yet
- RSCH2122 Inquiries WEEK 10 (1st Quarter Exam)Document6 pagesRSCH2122 Inquiries WEEK 10 (1st Quarter Exam)Christian PaulNo ratings yet
- Orca Share Media1682387604713 7056445059999513745Document54 pagesOrca Share Media1682387604713 7056445059999513745ALUNDAY, MELODY S.No ratings yet
- Ifx Midpoint EvaluationDocument7 pagesIfx Midpoint Evaluationapi-284751376No ratings yet
- Ass2 - Prefixes Suffixes - Lesson Plan 2Document3 pagesAss2 - Prefixes Suffixes - Lesson Plan 2api-267904090No ratings yet
- RQA TitleDocument13 pagesRQA TitleimpromtouNo ratings yet
- FARHAT ArticleDocument6 pagesFARHAT Articlefarhat najamNo ratings yet
- The MatsDocument3 pagesThe MatsReyniel VergaraNo ratings yet
- Week 6 Reflection BadmintonDocument3 pagesWeek 6 Reflection Badmintonapi-294958199No ratings yet
- j560 02 Paper 2 Foundation TierDocument20 pagesj560 02 Paper 2 Foundation TierEliotNo ratings yet
- PDAC-SEG Gold Deposits Curso Marzo 2011Document210 pagesPDAC-SEG Gold Deposits Curso Marzo 2011HenryOchoaSuarez100% (1)
- Chapter 3 - Eliciting RequiremnetsDocument61 pagesChapter 3 - Eliciting RequiremnetsKhairul Faris Bin OmarNo ratings yet
- The Little Brown HandbookDocument496 pagesThe Little Brown HandbookIrfan Ali100% (1)
- Literature Review PaperDocument13 pagesLiterature Review Paperapi-644641708No ratings yet
- Does A Dissertation Need A Literature ReviewDocument7 pagesDoes A Dissertation Need A Literature ReviewCustomPaperWritingNewark100% (1)
- Networking For VMware AdministratorsDocument369 pagesNetworking For VMware AdministratorsMohamad Reza Nazari100% (4)
- Day 1: Learning Engagement 1: The Role of The TeacherDocument4 pagesDay 1: Learning Engagement 1: The Role of The TeacherSBNo ratings yet
- The Self From Various Perspective PsychologyDocument36 pagesThe Self From Various Perspective PsychologyRhea Dela CruzNo ratings yet
- 3.an Unpleasant SurpriseDocument6 pages3.an Unpleasant SurprisemirfanulhaqNo ratings yet
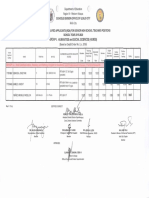
- HR Campus Tapping Database (Kerala)Document5 pagesHR Campus Tapping Database (Kerala)Divya GuptaNo ratings yet
- Sumit B.sc. 1st Year ResultDocument1 pageSumit B.sc. 1st Year ResultAmit kumar YadavNo ratings yet
- Advanced Condensed Matter Physics - Leonard M. SanderDocument288 pagesAdvanced Condensed Matter Physics - Leonard M. SanderSaagnik Paul100% (6)
- Resume 1Document2 pagesResume 1api-270710360No ratings yet
- Print and Power in Early Modern Europe (1500-1800) ) Print and Power in Early Modern Europe (1500-1800)Document461 pagesPrint and Power in Early Modern Europe (1500-1800) ) Print and Power in Early Modern Europe (1500-1800)Jaime Borja100% (1)
- Science Behind HugDocument4 pagesScience Behind HugNirav HiinguNo ratings yet
- Clase de Adscripción - PFDocument21 pagesClase de Adscripción - PFkNo ratings yet
- Principal of Lesson Planning: Stage 1: Pre-Lesson PreparationDocument6 pagesPrincipal of Lesson Planning: Stage 1: Pre-Lesson Preparationjaysel86No ratings yet