You might also like
- Guide to Title 24 Building Standards CodeDocument84 pagesGuide to Title 24 Building Standards CodeMich DeesNo ratings yet
- Achat Graded Health Policy Paper FinalDocument12 pagesAchat Graded Health Policy Paper Finalapi-339160012No ratings yet
- Capstone PaperDocument12 pagesCapstone Paperapi-315569993No ratings yet
- Health Policy PaperDocument11 pagesHealth Policy Paperapi-379546477No ratings yet
- Social Determinants in Health and InequalitiesDocument6 pagesSocial Determinants in Health and InequalitiesmartinsmariodamataNo ratings yet
- Compliance ChecklistDocument4 pagesCompliance ChecklistjpNo ratings yet
- Application PDFDocument6 pagesApplication PDFGezim DragociNo ratings yet
- Monthly Newborn Screening ReportDocument1 pageMonthly Newborn Screening ReportEarl Parungao50% (2)
- Gist of AP Budget 2019-20: Subscribe To IAS APPSC TSPSC Lectures Channel at YoutubeDocument18 pagesGist of AP Budget 2019-20: Subscribe To IAS APPSC TSPSC Lectures Channel at YoutuberushikeshNo ratings yet
- Health Policy Capstone PaperDocument15 pagesHealth Policy Capstone Paperapi-315208605No ratings yet
- Capstone SummativeDocument10 pagesCapstone Summativeapi-283153247No ratings yet
- Health Policy SummativeDocument13 pagesHealth Policy Summativeapi-364212510No ratings yet
- Hca300 Los Angeles Health Assessment 1Document12 pagesHca300 Los Angeles Health Assessment 1api-535414037No ratings yet
- Health Policy Paper Final DraftDocument16 pagesHealth Policy Paper Final Draftapi-457485362No ratings yet
- Nur4636 Health Policy Summative TTDocument15 pagesNur4636 Health Policy Summative TTapi-335042704No ratings yet
- Health Policy PaperDocument12 pagesHealth Policy Paperapi-485472556No ratings yet
- Health Policy SummativeDocument15 pagesHealth Policy Summativeapi-384129679No ratings yet
- Health Policy - Care Without Coverage FinalDocument8 pagesHealth Policy - Care Without Coverage Finalapi-362521769No ratings yet
- Health Policy Hillsborough CountyDocument14 pagesHealth Policy Hillsborough Countyapi-430800277No ratings yet
- Nguyen 1Document4 pagesNguyen 1api-302584213No ratings yet
- Health PolicyDocument15 pagesHealth Policyapi-438324478No ratings yet
- Health PolicyDocument14 pagesHealth Policyapi-373251639No ratings yet
- Community Demographics Paper RevisedDocument8 pagesCommunity Demographics Paper Revisedapi-341635920No ratings yet
- Obesity Summat IveDocument14 pagesObesity Summat IveKring Kring K. KringersNo ratings yet
- Running Head: Teen Birth Disparities in Sarasota 1Document15 pagesRunning Head: Teen Birth Disparities in Sarasota 1api-456052042No ratings yet
- Martinez Health Policy PaperDocument15 pagesMartinez Health Policy Paperapi-437349589No ratings yet
- 583 Writing AssignmentDocument9 pages583 Writing Assignmentapi-532105563No ratings yet
- CapstoneDocument11 pagesCapstoneMaureenAmilcaNo ratings yet
- Capstone Health Policy Paper - Kristina NealyDocument14 pagesCapstone Health Policy Paper - Kristina Nealyapi-314372295No ratings yet
- Capstone FormativeDocument12 pagesCapstone Formativeapi-300362033No ratings yet
- Capstone Paper FinalDocument12 pagesCapstone Paper Finalapi-302130584No ratings yet
- Capstone 1Document13 pagesCapstone 1api-314483635No ratings yet
- Population Analysis PaperDocument11 pagesPopulation Analysis Paperapi-285998412No ratings yet
- Health Policy PaperDocument13 pagesHealth Policy Paperapi-338998736No ratings yet
- Within The Hidden Epidemic: Sexually Transmitted Diseases and HIV/AIDS Among American Indians and Alaska NativesDocument11 pagesWithin The Hidden Epidemic: Sexually Transmitted Diseases and HIV/AIDS Among American Indians and Alaska NativesDarwinso AlvarezNo ratings yet
- Health Policy PaperDocument14 pagesHealth Policy Paperapi-433370150No ratings yet
- Food Insecurity in YpsilantiDocument17 pagesFood Insecurity in Ypsilantiapi-435449823No ratings yet
- Heart Disease in The Adult Population of Osceola CountyDocument10 pagesHeart Disease in The Adult Population of Osceola Countyapi-281676750No ratings yet
- Capstone Paper Project FormativeDocument11 pagesCapstone Paper Project Formativeapi-325259254No ratings yet
- Hep B FinalDocument12 pagesHep B Finalapi-315444338No ratings yet
- Capestone Paper Summitive FinalDocument12 pagesCapestone Paper Summitive Finalapi-302122563No ratings yet
- Community CapstoneDocument6 pagesCommunity Capstoneapi-641561231No ratings yet
- Teenage PregnancyDocument34 pagesTeenage Pregnancycc22santosNo ratings yet
- Research Paper DoneDocument12 pagesResearch Paper Doneapi-283540729No ratings yet
- Capstone PaperDocument8 pagesCapstone Paperapi-260053520No ratings yet
- Policy PaperDocument11 pagesPolicy Paperapi-679663498No ratings yet
- Population AnalysisDocument31 pagesPopulation AnalysisJoAnne SabaNo ratings yet
- Philippines Country Landscape OutlineDocument7 pagesPhilippines Country Landscape OutlineMa. Cristina TanadaNo ratings yet
- Community Cancer Capstone PaperDocument11 pagesCommunity Cancer Capstone Paperapi-283066063No ratings yet
- Step TemplateDocument41 pagesStep Templateapi-321260411100% (1)
- CHLH 575 Community Assessment 1Document3 pagesCHLH 575 Community Assessment 1api-338166341No ratings yet
- Capstone PaperDocument10 pagesCapstone Paperapi-294300618No ratings yet
- Group 3 Humss 12 JudgesDocument13 pagesGroup 3 Humss 12 JudgesMark HarryNo ratings yet
- Massachusetts Teen Births 2013Document18 pagesMassachusetts Teen Births 2013Patrick JohnsonNo ratings yet
- Assignment 1 Hsci 301Document4 pagesAssignment 1 Hsci 301api-301034352No ratings yet
- The Blueprint For Harm Reduction in Los Angeles - SampleDocument3 pagesThe Blueprint For Harm Reduction in Los Angeles - Samplepepper1955No ratings yet
- Community Capstone SummativeDocument9 pagesCommunity Capstone Summativeapi-283856107No ratings yet
- Health PolicyDocument13 pagesHealth Policyapi-403776891No ratings yet
- CHSI - BradleyDocument8 pagesCHSI - BradleyerlangerhealthNo ratings yet
- Making An Impact On Hispanic Community Health in Lehigh County, PennsylvaniaDocument8 pagesMaking An Impact On Hispanic Community Health in Lehigh County, PennsylvaniaTim RogersNo ratings yet
- Capstone PaperDocument9 pagesCapstone Paperapi-270783686No ratings yet
- Racial Disparities in Maternal and Infant Health_ An Overview – Issue Brief – 9577Document13 pagesRacial Disparities in Maternal and Infant Health_ An Overview – Issue Brief – 9577elenabarreto885No ratings yet
- CHSI Dade Co.Document8 pagesCHSI Dade Co.erlangerhealthNo ratings yet
- Community Capstone Health Policy PaperDocument17 pagesCommunity Capstone Health Policy Paperapi-417446716No ratings yet
- Medical Journal Block 4 2Document8 pagesMedical Journal Block 4 2aji argo putroNo ratings yet
- Clinical ExemplarDocument4 pagesClinical Exemplarapi-385494784No ratings yet
- FemaDocument1 pageFemaapi-385494784No ratings yet
- Brashears TaylorDocument3 pagesBrashears Taylorapi-385494784No ratings yet
- Jul 17 2018 at 6-19 PMDocument1 pageJul 17 2018 at 6-19 PMapi-385494784No ratings yet
- Upload1clabsi Qi PresentationfinalDocument13 pagesUpload1clabsi Qi Presentationfinalapi-385494784100% (1)
- GoalsDocument2 pagesGoalsapi-385494784No ratings yet
- Projectnurse UsfDocument5 pagesProjectnurse Usfapi-385494784No ratings yet
- Jul 17 2018 at 6-21 PMDocument1 pageJul 17 2018 at 6-21 PMapi-385494784No ratings yet
- 2 Ahec PharmacotherapyDocument1 page2 Ahec Pharmacotherapyapi-372188767No ratings yet
- Discharge Planning PaperDocument4 pagesDischarge Planning Paperapi-385494784No ratings yet
- Synthesis Paper SummativeDocument12 pagesSynthesis Paper Summativeapi-385494784No ratings yet
- Pat1 2Document16 pagesPat1 2api-385494784No ratings yet
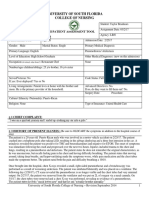
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument21 pagesUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-385494784No ratings yet
- Philippine Health Care Providers, Inc.: Commissioner of Internal RevenueDocument17 pagesPhilippine Health Care Providers, Inc.: Commissioner of Internal RevenuePatricia Ann Nicole ReyesNo ratings yet
- Al Sharpton For de BlasioDocument2 pagesAl Sharpton For de BlasioAzi PaybarahNo ratings yet
- Business Ethics & Social ResponsibilityDocument18 pagesBusiness Ethics & Social ResponsibilitySangeethaNo ratings yet
- Session 3 Life Insurance Products: Conventional Plans - Non Participating PlansDocument30 pagesSession 3 Life Insurance Products: Conventional Plans - Non Participating Plansm_dattaiasNo ratings yet
- S.No Designation/Role Representing Organisation/ InstitutionDocument56 pagesS.No Designation/Role Representing Organisation/ InstitutionRamprasath JayabalanNo ratings yet
- Tricare Participation FormDocument8 pagesTricare Participation FormMalsom SingsonNo ratings yet
- Minister of Health V TreatmentDocument82 pagesMinister of Health V TreatmentABDOULIENo ratings yet
- Glossary: Agency - Certified Home Health Care Agencies. Certified Home Health AgenciesDocument8 pagesGlossary: Agency - Certified Home Health Care Agencies. Certified Home Health AgenciesLinda RodriguezNo ratings yet
- Schilling GT DisciplinaryDocument9 pagesSchilling GT DisciplinaryDan LehrNo ratings yet
- War's Offensive On Women - The Humanitarian Challenge in Bosnia, Kosovo, and Afghanistan by Julie A. Mertus (2000)Document176 pagesWar's Offensive On Women - The Humanitarian Challenge in Bosnia, Kosovo, and Afghanistan by Julie A. Mertus (2000)Anonymous yu09qxYCM100% (1)
- Fall Rally Permission Form 2017Document2 pagesFall Rally Permission Form 2017api-306130000No ratings yet
- Act 350 - Children and Young Persons (Employment) Act 1966Document21 pagesAct 350 - Children and Young Persons (Employment) Act 1966hakimi83No ratings yet
- Citizens Response and Arguments Against Closing Muhlenberg HospitalDocument15 pagesCitizens Response and Arguments Against Closing Muhlenberg HospitalDeborah Joyce DoweNo ratings yet
- Workshop Accomplishment Report For SubmissionDocument16 pagesWorkshop Accomplishment Report For SubmissionTata CarreonNo ratings yet
- Westchester Overtime Costs MillionsDocument2 pagesWestchester Overtime Costs MillionsGerald McKinstryNo ratings yet
- Annual Premium Statement: Nagarajan KDocument1 pageAnnual Premium Statement: Nagarajan KRajanNo ratings yet
- Guidelines For The Mnagement of Safety For Construction Work in ODA Projects Vol 1-3Document211 pagesGuidelines For The Mnagement of Safety For Construction Work in ODA Projects Vol 1-3lwin_oo2435No ratings yet
- The Independent Issue 546Document44 pagesThe Independent Issue 546The Independent MagazineNo ratings yet
- Notice of Cmucat Result: Central Mindanao UniversityDocument2 pagesNotice of Cmucat Result: Central Mindanao UniversityLANI JOY TABAMONo ratings yet
- Living Will...Document14 pagesLiving Will...gilbertmalcolmNo ratings yet
- Principles For Hot Work On Board All Types of ShipDocument2 pagesPrinciples For Hot Work On Board All Types of ShipkfidiantoroNo ratings yet
- A Project On Quiz On Indian Labour LawsDocument258 pagesA Project On Quiz On Indian Labour LawsMohammad ShoebNo ratings yet
- Everyday Heroes 2017Document16 pagesEveryday Heroes 2017The Standard NewspaperNo ratings yet