You might also like
- Shoulder DislocationDocument6 pagesShoulder DislocationRizki IrwansyahNo ratings yet
- APJCP - Volume 16 - Issue 18 - Pages 8141-8143 PDFDocument3 pagesAPJCP - Volume 16 - Issue 18 - Pages 8141-8143 PDFRizki IrwansyahNo ratings yet
- Helicobacter A Paradigm ShiftDocument20 pagesHelicobacter A Paradigm ShiftRizki IrwansyahNo ratings yet
- The Elements of Fracture Fixation 2nd EdDocument13 pagesThe Elements of Fracture Fixation 2nd EdRizki Irwansyah0% (2)
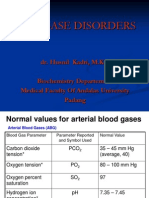
- Acid Base DisordersDocument28 pagesAcid Base DisordersRizki IrwansyahNo ratings yet
- DSTC LDocument465 pagesDSTC LRizki Irwansyah100% (2)
- Worksheets EBMDocument19 pagesWorksheets EBMRizki IrwansyahNo ratings yet
- Constipation in Children (Functional or Anatomical)Document23 pagesConstipation in Children (Functional or Anatomical)Rizki IrwansyahNo ratings yet
- CT ScanDocument4 pagesCT ScanRizki IrwansyahNo ratings yet
- Red Eye DDDocument33 pagesRed Eye DDRizki IrwansyahNo ratings yet
- The One That Got AwayDocument5 pagesThe One That Got AwayRizki Irwansyah100% (1)
- Jay Sean-Down Piano CoverDocument9 pagesJay Sean-Down Piano CoverJun Hao HengNo ratings yet
- List Top GameDocument1 pageList Top GameRizki IrwansyahNo ratings yet
- Vaginal Birth After Cesarean: New Insights: Evidence Report/Technology AssessmentDocument397 pagesVaginal Birth After Cesarean: New Insights: Evidence Report/Technology AssessmentRizki IrwansyahNo ratings yet
- Hypertension and PregnancyDocument1 pageHypertension and PregnancyRizki IrwansyahNo ratings yet
- Jay Sean - TonightDocument3 pagesJay Sean - TonightRizki IrwansyahNo ratings yet
- Body Surface AreaDocument2 pagesBody Surface AreaRizki IrwansyahNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- HAAD Exams Schedule 2Document1 pageHAAD Exams Schedule 2a2u2No ratings yet
- Decent 6Document3 pagesDecent 6Han Joshua PacañaNo ratings yet
- Healthy Women Healthy Economies: A Look at BrazilDocument10 pagesHealthy Women Healthy Economies: A Look at BrazilThe Wilson CenterNo ratings yet
- JI ManifestoDocument32 pagesJI ManifestoHussain AfzalNo ratings yet
- Non-Operating Room Anesthesia (NORA) : A Beginner's GuideDocument26 pagesNon-Operating Room Anesthesia (NORA) : A Beginner's GuidepaulaNo ratings yet
- Ethical Dilemmas of End of Life Care in Intensive Care Unit: A Literature ReviewDocument9 pagesEthical Dilemmas of End of Life Care in Intensive Care Unit: A Literature ReviewEviNo ratings yet
- Public Health Delivery The Role of Informatics and TechnologyDocument19 pagesPublic Health Delivery The Role of Informatics and Technologysbaracaldo2No ratings yet
- Dr. Deshinta - Adult Vaccination Pontianak PDFDocument38 pagesDr. Deshinta - Adult Vaccination Pontianak PDFIzka P RahmaniaNo ratings yet
- 2017 Implant Aesthetics - Keys To Diagnosis and TreatmentDocument453 pages2017 Implant Aesthetics - Keys To Diagnosis and TreatmentbetsaNo ratings yet
- Management Programmes: Certificate in ComputersDocument3 pagesManagement Programmes: Certificate in ComputersPriyanka MehtaNo ratings yet
- RA 9994. Expanded Senior Citizens Act of 2010Document12 pagesRA 9994. Expanded Senior Citizens Act of 2010Miamor NatividadNo ratings yet
- DAFTAR HADIR KARYAWAN PUSKESMASDocument65 pagesDAFTAR HADIR KARYAWAN PUSKESMASLaela YusrianaNo ratings yet
- DR Prathap C ReddyDocument2 pagesDR Prathap C ReddyApollo HospitalsNo ratings yet
- SRF ID COVID-19 Test DetailsDocument2 pagesSRF ID COVID-19 Test DetailsShruti JainNo ratings yet
- PMFIAS CA 2019 05 12 SciDocument107 pagesPMFIAS CA 2019 05 12 SciShivy SwarnkarNo ratings yet
- Hope Mcmullin Resume 3-26-23Document3 pagesHope Mcmullin Resume 3-26-23api-659960796No ratings yet
- DR UsmanDocument7 pagesDR Usmanusman_rana84No ratings yet
- 1320-Doctors in Sweden Say There Is A Cure For ArthritisDocument5 pages1320-Doctors in Sweden Say There Is A Cure For Arthritisguapo210% (1)
- Davao Doctors College Nursing Graduates EmployabilityDocument130 pagesDavao Doctors College Nursing Graduates EmployabilityMelanie GaledoNo ratings yet
- Blair County Community ResourcesDocument6 pagesBlair County Community Resourcesapi-245261928No ratings yet
- Jamda: Richard M. Lynch PHD, Reginald Goring BsDocument2 pagesJamda: Richard M. Lynch PHD, Reginald Goring BsWidarma Atmaja, I KomangNo ratings yet
- CPR Instruction SetDocument6 pagesCPR Instruction SetKatelyn CherryNo ratings yet
- Cochrane Report - Phase 2Document112 pagesCochrane Report - Phase 2Omar Ha-RedeyeNo ratings yet
- Unit Test in MAPEH 2nd Quarter 18 19Document3 pagesUnit Test in MAPEH 2nd Quarter 18 19Joshua CasemNo ratings yet
- Erin Wesolowski Resume 2021Document2 pagesErin Wesolowski Resume 2021api-544181914No ratings yet
- Counseling HIV/AIDS PatientsDocument3 pagesCounseling HIV/AIDS PatientsYc ChingtonNo ratings yet
- Telemedicine Seminar HMTI v1.5Document25 pagesTelemedicine Seminar HMTI v1.5PriaTongNo ratings yet
- Pengaruh Kombinasi Pursed-Lip Breathing Dan Guided Imagery Music TerhadapDocument7 pagesPengaruh Kombinasi Pursed-Lip Breathing Dan Guided Imagery Music TerhadapFaisal AmirNo ratings yet
- Introduction To Regulatory AffairsDocument15 pagesIntroduction To Regulatory AffairsCyclone Pharmaceuticals Pvt Ltd PuneNo ratings yet
- BC prescription drug regulations summaryDocument2 pagesBC prescription drug regulations summaryRicky TsuiNo ratings yet