You might also like
- QBP KidneyDocument36 pagesQBP KidneyRaka ArifirmandaNo ratings yet
- Methods For Reticulocyte CountingDocument52 pagesMethods For Reticulocyte CountingAri EcheverríaNo ratings yet
- Clinical Trial ProtocolDocument30 pagesClinical Trial Protocolanand kumar gondNo ratings yet
- Research Design in Health Services and Health PolicyDocument4 pagesResearch Design in Health Services and Health PolicyrealsilverleNo ratings yet
- JURNALDocument12 pagesJURNALAsMiraaaaNo ratings yet
- Key Terms of EHRs and Examples in Various Types of Care SettingsDocument10 pagesKey Terms of EHRs and Examples in Various Types of Care SettingsDariaZhuravlevaNo ratings yet
- Bhutan National Standards BT ServicesDocument98 pagesBhutan National Standards BT ServicesDarla YsavelNo ratings yet
- Clinical Pathways Frequently Asked QuestionsDocument8 pagesClinical Pathways Frequently Asked Questionsagung kurniaNo ratings yet
- Understanding Clinical Trial LingoDocument36 pagesUnderstanding Clinical Trial Lingojram00No ratings yet
- Avoiding Bias in Selecting StudiesDocument26 pagesAvoiding Bias in Selecting StudiesOsama MohamedNo ratings yet
- Abcs Toolkit 2016Document176 pagesAbcs Toolkit 2016Kristen LynchNo ratings yet
- Arnold Ventures FDA Draft Guidance DCT Aug 2023Document3 pagesArnold Ventures FDA Draft Guidance DCT Aug 2023Arnold VenturesNo ratings yet
- Perit Dial Int 2011 Blake 218 39Document22 pagesPerit Dial Int 2011 Blake 218 39Ika AgustinNo ratings yet
- Article Managing Effective QueryDocument10 pagesArticle Managing Effective QueryKenpachi23No ratings yet
- 151 Nursing DocumentationDocument24 pages151 Nursing DocumentationNasrullah UllahNo ratings yet
- ICU Report ENDocument36 pagesICU Report ENEmilio AcostaNo ratings yet
- Pegels Et Al 1977Document12 pagesPegels Et Al 1977Virgínia MagalhãesNo ratings yet
- s12882 020 1683 5Document10 pagess12882 020 1683 5arifin hidayatNo ratings yet
- Pubs CatalogDocument36 pagesPubs CatalogMohamed EltonsyNo ratings yet
- Standard Operating Proceduresgov1Document197 pagesStandard Operating Proceduresgov1Adam ShawNo ratings yet
- Prosthesis Draft ReportDocument440 pagesProsthesis Draft ReportMuhammad ZawarNo ratings yet
- Aabb User Guide: Circular of Information For The Use of Human Blood and Blood Components October, 2017 AcknowledgementsDocument8 pagesAabb User Guide: Circular of Information For The Use of Human Blood and Blood Components October, 2017 AcknowledgementsdamadolNo ratings yet
- GST FusionDocument28 pagesGST FusionBabbooNo ratings yet
- Guidelines For Achieving A Compliant Query PracticeDocument10 pagesGuidelines For Achieving A Compliant Query PracticeKenpachi23No ratings yet
- Locating Credible Databases and ResearchDocument7 pagesLocating Credible Databases and ResearchTrex WritersNo ratings yet
- Hemodialysis PDFDocument244 pagesHemodialysis PDFMorrison Njage100% (1)
- Cber Safety Initiatives-Blood Safety Team CRF PDFDocument13 pagesCber Safety Initiatives-Blood Safety Team CRF PDFgpNo ratings yet
- Hastane SeçimiDocument16 pagesHastane Seçimiİbrahim GüçlüNo ratings yet
- Imaging Safety InformationDocument20 pagesImaging Safety InformationAbouzr Mohammed ElsaidNo ratings yet
- P-O Research Strategy-EngDocument40 pagesP-O Research Strategy-EngSheila SchneibergNo ratings yet
- FDA Inspections of Clinical InvestigatorsDocument9 pagesFDA Inspections of Clinical InvestigatorsJudit SzepesiNo ratings yet
- CAHPS Patient Survey Program BriefDocument6 pagesCAHPS Patient Survey Program BriefAlaa AhmedNo ratings yet
- Pediatric Cancer SurvivorshipDocument315 pagesPediatric Cancer SurvivorshipRJ HSNo ratings yet
- Creating A Library of Patient Registry Metrics For Quality ImprovementDocument13 pagesCreating A Library of Patient Registry Metrics For Quality Improvementapi-529619824No ratings yet
- Technical Brief 31 - Mobile Health Applications For Self Management of DiabetesDocument73 pagesTechnical Brief 31 - Mobile Health Applications For Self Management of DiabetesYaser ZaherNo ratings yet
- FelowshipalbertaDocument10 pagesFelowshipalbertaclaudiaNo ratings yet
- Guide To Writing Grant ProposalsDocument15 pagesGuide To Writing Grant ProposalsMartina NoelNo ratings yet
- Improving Health CareDocument249 pagesImproving Health CareDiandhara Nuryadin100% (1)
- Hipo - Hiper SubDocument123 pagesHipo - Hiper SubdankouzielNo ratings yet
- Social Determinants of Health. Training 042815Document57 pagesSocial Determinants of Health. Training 042815Jenine's Handmade SoapNo ratings yet
- Navigating the Medical RecordDocument28 pagesNavigating the Medical RecordMiranda Robledo Amezcua0% (1)
- B. What Is A SOAP Note? Define Each ComponentDocument3 pagesB. What Is A SOAP Note? Define Each ComponentNeth MerquitaNo ratings yet
- Good Abbreviated New Drug Application Assessment Practices MAPP 5241.3 2018-01-03Document11 pagesGood Abbreviated New Drug Application Assessment Practices MAPP 5241.3 2018-01-03Markbot1999No ratings yet
- Standard Operating Procedure for Source DocumentationDocument29 pagesStandard Operating Procedure for Source DocumentationSreeraj Guruvayoor SNo ratings yet
- GCLPDocument116 pagesGCLPLordie Jordan Nalus100% (1)
- Defensible Documentation Quick ReferenceDocument3 pagesDefensible Documentation Quick ReferencecderdnaseNo ratings yet
- CDRH2011111 CompanionDx Final Guidance 7-24-14 PDFDocument13 pagesCDRH2011111 CompanionDx Final Guidance 7-24-14 PDFstalker1841No ratings yet
- The Sourcebook for Clinical Research: A Practical Guide for Study ConductFrom EverandThe Sourcebook for Clinical Research: A Practical Guide for Study ConductRating: 5 out of 5 stars5/5 (1)
- Blood Admin Addendum 2012Document4 pagesBlood Admin Addendum 2012Sanjeewa WijayawickramaNo ratings yet
- Project Proposal - Online Blood Bank MisDocument15 pagesProject Proposal - Online Blood Bank MisYvesMKNo ratings yet
- HCVGuidance September 21 2017 GDocument241 pagesHCVGuidance September 21 2017 GDM internaNo ratings yet
- UNIT-5-CLINICAL-DATA-REPOSITORIES Public Health - RemovedDocument10 pagesUNIT-5-CLINICAL-DATA-REPOSITORIES Public Health - RemovedKelvin CafirmaNo ratings yet
- How To Prepare and Present La Evidencia A ConsumidoresDocument39 pagesHow To Prepare and Present La Evidencia A ConsumidoresogianneoNo ratings yet
- Transfusion-Free Medicine and SurgeryFrom EverandTransfusion-Free Medicine and SurgeryNicolas JabbourNo ratings yet
- Equine Clinical PathologyFrom EverandEquine Clinical PathologyRaquel M. WaltonNo ratings yet
- Biomarkers, Diagnostics and Precision Medicine in the Drug Industry: Critical Challenges, Limitations and Roadmaps for the Best PracticesFrom EverandBiomarkers, Diagnostics and Precision Medicine in the Drug Industry: Critical Challenges, Limitations and Roadmaps for the Best PracticesNo ratings yet
- Untitled Document PDFDocument1 pageUntitled Document PDFMary Joyce AngalaNo ratings yet
- Second Floor Power and Auxiliary Layout: D E F G H I J K L A B CDocument1 pageSecond Floor Power and Auxiliary Layout: D E F G H I J K L A B CMary Joyce AngalaNo ratings yet
- First Floor Drainage System: D E F G H I J K L A B CDocument1 pageFirst Floor Drainage System: D E F G H I J K L A B CMary Joyce AngalaNo ratings yet
- First Floor Water Supply Layout: D E F G H I J K L A B CDocument1 pageFirst Floor Water Supply Layout: D E F G H I J K L A B CMary Joyce AngalaNo ratings yet
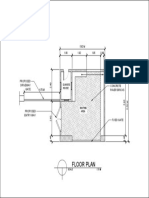
- Proposed floor plan for a guard house and drivewayDocument1 pageProposed floor plan for a guard house and drivewayMary Joyce AngalaNo ratings yet
- Single Line Diagram: General NotesDocument1 pageSingle Line Diagram: General NotesMary Joyce AngalaNo ratings yet
- Hypertension Drugs Cheat Sheet: by ViaDocument3 pagesHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharNo ratings yet
- Fundamentals of Occlusion and Restorative DentistryDocument9 pagesFundamentals of Occlusion and Restorative Dentistrypablo_elguezábalNo ratings yet
- The Tocqueville Review/La Revue Tocqueville, Vol. XXVII, N° 2 - 2006Document16 pagesThe Tocqueville Review/La Revue Tocqueville, Vol. XXVII, N° 2 - 2006Valente EnacheNo ratings yet
- EV3110 SIA Group ReportDocument38 pagesEV3110 SIA Group ReportWill MyatNo ratings yet
- MudreDocument10 pagesMudrejezebelvertNo ratings yet
- Tingkat KesadaranDocument16 pagesTingkat KesadaranShinta NurjanahNo ratings yet
- Karen Horney, Self-Analysis, 1942Document312 pagesKaren Horney, Self-Analysis, 1942Brian EverettNo ratings yet
- UPS MaintenanceDocument3 pagesUPS MaintenancedescslamNo ratings yet
- Tugas Parafrase Jurnal MIPKI (Revisi) - Rizka Amalia Hutami - 150510160235Document2 pagesTugas Parafrase Jurnal MIPKI (Revisi) - Rizka Amalia Hutami - 150510160235RizkaNo ratings yet
- Facts of MaintenanceDocument9 pagesFacts of Maintenancegeorge youssefNo ratings yet
- Resolve Family Drainage CatetherDocument16 pagesResolve Family Drainage CatetherradeonunNo ratings yet
- Syllabus ECDO 4225 - Professional Aspects of Nutrition and DieteticsDocument6 pagesSyllabus ECDO 4225 - Professional Aspects of Nutrition and DieteticsOEAENo ratings yet
- CG A022 01 Shortened Dental ArchDocument5 pagesCG A022 01 Shortened Dental ArchmahmoudNo ratings yet
- 4bi1 - Jan22 2b QPDocument28 pages4bi1 - Jan22 2b QPXIN PEINo ratings yet
- BS EN 752-2 Drains & Sewer PDFDocument21 pagesBS EN 752-2 Drains & Sewer PDFsefaz50% (2)
- Methods of Investigating Brain and LanguageDocument12 pagesMethods of Investigating Brain and Languagekiranjit_123100% (2)
- StramoniumDocument114 pagesStramoniumJoão FrancoNo ratings yet
- "PASS" Principles For Predictable PDFDocument10 pages"PASS" Principles For Predictable PDFkishan bordaNo ratings yet
- ICU antibiotic susceptibilities guideDocument1 pageICU antibiotic susceptibilities guideFaisal Reza AdiebNo ratings yet
- EN Sample Paper 12 UnsolvedDocument9 pagesEN Sample Paper 12 Unsolvedguptasubhanjali21No ratings yet
- SGLGB Form 1 Barangay ProfileDocument3 pagesSGLGB Form 1 Barangay ProfileMark Lenon Par Mapaye100% (1)
- Updates On Upper Eyelid Blepharoplasty.4Document8 pagesUpdates On Upper Eyelid Blepharoplasty.4Dimitris RodriguezNo ratings yet
- Wellness ChallengeDocument2 pagesWellness ChallengemeganbastianNo ratings yet
- Speaking Level Placement Test Business English PDFDocument2 pagesSpeaking Level Placement Test Business English PDFLee HarrisonNo ratings yet
- Case Control Study For MedicDocument41 pagesCase Control Study For Medicnunu ahmedNo ratings yet
- UserGuide2015 PDFDocument114 pagesUserGuide2015 PDFYihan WangNo ratings yet
- L-Sit ProgressionsDocument2 pagesL-Sit ProgressionsMattNo ratings yet
- Radiographic Cardiopulmonary Changes in Dogs With Heartworm DiseaseDocument8 pagesRadiographic Cardiopulmonary Changes in Dogs With Heartworm DiseaseputriwilujengNo ratings yet
- Ultra Shred Workout (By Brian Jung)Document10 pagesUltra Shred Workout (By Brian Jung)sannaluizazampro0100% (1)
- Curriculum Map Grade 9 Health: T (N .) M U T C C S P S C S A A R I C V Quarter 1Document5 pagesCurriculum Map Grade 9 Health: T (N .) M U T C C S P S C S A A R I C V Quarter 1joan niniNo ratings yet