You might also like
- Psychology 2 Test #2 Study GuideDocument10 pagesPsychology 2 Test #2 Study GuideIqbal BaryarNo ratings yet
- Psych 2 Practice TestDocument9 pagesPsych 2 Practice TestIqbal BaryarNo ratings yet
- Significant Variables That Influence Psychotherapy PDFDocument38 pagesSignificant Variables That Influence Psychotherapy PDFIqbal BaryarNo ratings yet
- Significant Variables That Influence Psychotherapy PDFDocument38 pagesSignificant Variables That Influence Psychotherapy PDFIqbal BaryarNo ratings yet
- DocuNotes Clinical Pocket Guide To Effective ChartingDocument203 pagesDocuNotes Clinical Pocket Guide To Effective ChartingShirlyn Ares Navarro96% (47)
- SW112 Lecture on Poverty Rate, Public Assistance ProgramsDocument2 pagesSW112 Lecture on Poverty Rate, Public Assistance ProgramsIqbal BaryarNo ratings yet
- 11.10psych 101 LectureDocument1 page11.10psych 101 LectureIqbal BaryarNo ratings yet
- 11.29 Chapter 21 Nonparametric TestsDocument1 page11.29 Chapter 21 Nonparametric TestsIqbal BaryarNo ratings yet
- Psych 2 Practice TestDocument9 pagesPsych 2 Practice TestIqbal BaryarNo ratings yet
- ANOVA Tests-Psych 101Document2 pagesANOVA Tests-Psych 101Iqbal BaryarNo ratings yet
- 11.27 SW 112 LectureDocument1 page11.27 SW 112 LectureIqbal BaryarNo ratings yet
- Interpretation of Hepatitis B Serologic Test ResultsDocument1 pageInterpretation of Hepatitis B Serologic Test ResultsMUHAMMAD JAWAD HASSANNo ratings yet
- 11.20 SW 112 LectureDocument5 pages11.20 SW 112 LectureIqbal BaryarNo ratings yet
- 11.29 Chapter 21 Nonparametric TestsDocument1 page11.29 Chapter 21 Nonparametric TestsIqbal BaryarNo ratings yet
- Psych 2-Chapter 14 Answer KeyDocument1 pagePsych 2-Chapter 14 Answer KeyIqbal BaryarNo ratings yet
- Psych 2-Chapter 13 Practice TestDocument4 pagesPsych 2-Chapter 13 Practice TestIqbal BaryarNo ratings yet
- User Guide Nokia 3310 User GuideDocument59 pagesUser Guide Nokia 3310 User GuideIqbal BaryarNo ratings yet
- Psych 2 Test #1 Answer KeyDocument2 pagesPsych 2 Test #1 Answer KeyIqbal BaryarNo ratings yet
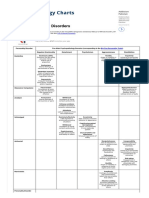
- DSM-5 List of Mental DisordersDocument2 pagesDSM-5 List of Mental DisordersIqbal Baryar100% (1)
- Addiction Rehab Pakistan Evidence-Based TreatmentDocument2 pagesAddiction Rehab Pakistan Evidence-Based TreatmentIqbal Baryar0% (1)
- Introduction To Psychology: PsychopathologyDocument56 pagesIntroduction To Psychology: PsychopathologyIqbal Baryar100% (1)
- Introduction To Psychology: Social Influences and RelationshipsDocument36 pagesIntroduction To Psychology: Social Influences and RelationshipsIqbal Baryar100% (1)
- Introduction To Psychology: Social DevelopmentDocument22 pagesIntroduction To Psychology: Social DevelopmentIqbal BaryarNo ratings yet
- DSM-5 Personality DisordersDocument2 pagesDSM-5 Personality DisordersIqbal BaryarNo ratings yet
- DSM-5 Personality DisordersDocument2 pagesDSM-5 Personality DisordersIqbal Baryar100% (1)
- DBT Therapy - Dialectical Behavior TherapyDocument3 pagesDBT Therapy - Dialectical Behavior TherapyIqbal Baryar100% (2)
- Adult Neurological QuestionnaireDocument1 pageAdult Neurological QuestionnaireIqbal BaryarNo ratings yet
- General Health QuestionnaireDocument1 pageGeneral Health QuestionnaireIqbal Baryar83% (6)
- Stranger Harassment Inde1Document1 pageStranger Harassment Inde1Iqbal BaryarNo ratings yet
- Screening Tool for Drug Abuse (DASTDocument1 pageScreening Tool for Drug Abuse (DASTCesar OstolazaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ScriptDocument12 pagesScriptWaleed Nadeem50% (2)
- Ethics For Hospital AdministrationDocument46 pagesEthics For Hospital AdministrationAnonymous ibmeej9100% (3)
- Workshop Scientific WritingDocument27 pagesWorkshop Scientific WritingspiderNo ratings yet
- BUP Entrepreneurship Course OutlineDocument4 pagesBUP Entrepreneurship Course OutlineRahiq AhmedNo ratings yet
- CV - Anders BergmanDocument2 pagesCV - Anders BergmanAndersFuturegamesNo ratings yet
- A Foursquare "Church by The Highway" Draft Program Manual: VisionDocument23 pagesA Foursquare "Church by The Highway" Draft Program Manual: VisionPtr MarsNo ratings yet
- Dream It, Do It, Live It: 9 Easy Steps To Making Things Happen For YouDocument23 pagesDream It, Do It, Live It: 9 Easy Steps To Making Things Happen For YouCapstone PublishingNo ratings yet
- Employee Reprimand Letter for TardinessDocument4 pagesEmployee Reprimand Letter for TardinessMarjoriz Tan Ignacio100% (1)
- Six Circles - An Experience Design FrameworkDocument50 pagesSix Circles - An Experience Design FrameworkJames Kelway100% (4)
- Communicating EffectivelyDocument3 pagesCommunicating EffectivelyChong Hong SiaNo ratings yet
- History of Language TeachingDocument14 pagesHistory of Language TeachingRia RarasatiNo ratings yet
- The Weight of The GlassDocument2 pagesThe Weight of The GlassLINDANo ratings yet
- Introduction To Personal DevelopmentDocument3 pagesIntroduction To Personal DevelopmentGwen MagtabogNo ratings yet
- Elder MistreatmentDocument39 pagesElder MistreatmentDoha EbedNo ratings yet
- Re - ZERO - Starting Life in Another World-, Vol. 13 PDFDocument266 pagesRe - ZERO - Starting Life in Another World-, Vol. 13 PDFSharathKumar100% (1)
- Factors Affecting Organizational Citizenship Behavior of Port Authority Staff at Tanjung Priok PortDocument10 pagesFactors Affecting Organizational Citizenship Behavior of Port Authority Staff at Tanjung Priok PortGud SangadNo ratings yet
- Table of Specifications: 2019-2020 No. of Test Items Remembering Understandin G Applying Analyzing Evaluating CreatingDocument1 pageTable of Specifications: 2019-2020 No. of Test Items Remembering Understandin G Applying Analyzing Evaluating CreatingErich AgustinNo ratings yet
- Mandela Leadership TheoryDocument27 pagesMandela Leadership TheoryLOVERS NGOBENINo ratings yet
- Kenya HRH Strategic Plan 2009-2012Document72 pagesKenya HRH Strategic Plan 2009-2012k_hadharmy1653No ratings yet
- Daily Lesson Plan on Thesis StatementsDocument4 pagesDaily Lesson Plan on Thesis StatementsKanon NakanoNo ratings yet
- Exploring The Differences Between Discussion, Debate, and DialogueDocument2 pagesExploring The Differences Between Discussion, Debate, and Dialogueعطية الأوجليNo ratings yet
- Wood Skills Program LomandraDocument5 pagesWood Skills Program Lomandraapi-254931477No ratings yet
- DerridaDocument7 pagesDerridaUmesh KaisthaNo ratings yet
- Human Resource PlanningDocument62 pagesHuman Resource PlanningDeepakkr2510100% (2)
- (ENT) 1.03 Inner Ear (Part 2) Basic Concepts of Hearing Loss and Aural Rehabilitation - Dr. LagoDocument7 pages(ENT) 1.03 Inner Ear (Part 2) Basic Concepts of Hearing Loss and Aural Rehabilitation - Dr. LagoDenise CedeñoNo ratings yet
- Book of ThoughtsDocument20 pagesBook of ThoughtsNIWEWE David100% (1)
- BetaCodex-OrgPhysic Niels PflaegingDocument27 pagesBetaCodex-OrgPhysic Niels PflaegingClaudia TirbanNo ratings yet
- Elizabeth F Loftus-Memory, Surprising New Insights Into How We Remember and Why We forget-Addison-Wesley Pub. Co (1980) PDFDocument225 pagesElizabeth F Loftus-Memory, Surprising New Insights Into How We Remember and Why We forget-Addison-Wesley Pub. Co (1980) PDFAbraham VidalNo ratings yet
- Violence Against WomenDocument14 pagesViolence Against Womenlachel joy tahinayNo ratings yet