You might also like
- Podj 3 PDFDocument2 pagesPodj 3 PDFwennyNo ratings yet
- Produce101s2 PDFDocument22 pagesProduce101s2 PDFwennyNo ratings yet
- Oral Pathology - Clinical Pathologic Correlations - 6th - EdDocument4 pagesOral Pathology - Clinical Pathologic Correlations - 6th - EdwennyNo ratings yet
- Textbook of Oral Medicine PDFDocument1,179 pagesTextbook of Oral Medicine PDFwenny100% (1)
- Sist. Urine 2015 2Document37 pagesSist. Urine 2015 2wennyNo ratings yet
- AG C O L: Uide To Ommon RAL EsionsDocument46 pagesAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanNo ratings yet
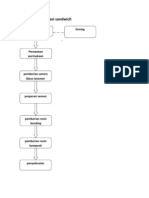
- Teknik dan bahan restorasi sandwichDocument6 pagesTeknik dan bahan restorasi sandwichMaria Apriliana100% (1)
- Handbook of Oral Diseases 1 Edition PDFDocument30 pagesHandbook of Oral Diseases 1 Edition PDFwennyNo ratings yet
- 4Document5 pages4wennyNo ratings yet
- GypsumDocument14 pagesGypsummuskanNo ratings yet
- AG C O L: Uide To Ommon RAL EsionsDocument46 pagesAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanNo ratings yet
- GypsumDocument14 pagesGypsummuskanNo ratings yet
- Geographic TongueDocument2 pagesGeographic TonguewennyNo ratings yet
- Geographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewDocument12 pagesGeographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewwennyNo ratings yet
- Geographic Tongue: Clinical Characteristics of 188 CasesDocument11 pagesGeographic Tongue: Clinical Characteristics of 188 CaseswennyNo ratings yet
- Geographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewDocument12 pagesGeographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewwennyNo ratings yet
- Immunology Dental CariesDocument24 pagesImmunology Dental CarieswennyNo ratings yet
- Dental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteratureDocument6 pagesDental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteraturewennyNo ratings yet
- AG C O L: Uide To Ommon RAL EsionsDocument46 pagesAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- A Review On Translation Strategies of Little Prince' by Ahmad Shamlou and Abolhasan NajafiDocument9 pagesA Review On Translation Strategies of Little Prince' by Ahmad Shamlou and Abolhasan Najafiinfo3814No ratings yet
- FPR 10 1.lectDocument638 pagesFPR 10 1.lectshishuNo ratings yet
- 05 Gregor and The Code of ClawDocument621 pages05 Gregor and The Code of ClawFaye Alonzo100% (7)
- The Serpents Tail A Brief History of KHMDocument294 pagesThe Serpents Tail A Brief History of KHMWill ConquerNo ratings yet
- MatriarchyDocument11 pagesMatriarchyKristopher Trey100% (1)
- Exámenes Trinity C1 Ejemplos - Modelo Completos de Examen PDFDocument6 pagesExámenes Trinity C1 Ejemplos - Modelo Completos de Examen PDFM AngelesNo ratings yet
- Microsoft Word - G10 Workbook - Docx 7Document88 pagesMicrosoft Word - G10 Workbook - Docx 7Pax TonNo ratings yet
- Explaining ADHD To TeachersDocument1 pageExplaining ADHD To TeachersChris100% (2)
- P.E 4 Midterm Exam 2 9Document5 pagesP.E 4 Midterm Exam 2 9Xena IngalNo ratings yet
- Tutorial Basico Del Metodo AJAX Con PHP y MySQLDocument14 pagesTutorial Basico Del Metodo AJAX Con PHP y MySQLJeese Bahena GarciaNo ratings yet
- Developments in ESP: A Multi-Disciplinary ApproachDocument12 pagesDevelopments in ESP: A Multi-Disciplinary ApproachDragana Lorelai JankovicNo ratings yet
- MC-SUZUKI@LS 650 (F) (P) @G J K L M R@601-750cc@175Document103 pagesMC-SUZUKI@LS 650 (F) (P) @G J K L M R@601-750cc@175Lanz Silva100% (1)
- Opportunity, Not Threat: Crypto AssetsDocument9 pagesOpportunity, Not Threat: Crypto AssetsTrophy NcNo ratings yet
- UG022510 International GCSE in Business Studies 4BS0 For WebDocument57 pagesUG022510 International GCSE in Business Studies 4BS0 For WebAnonymous 8aj9gk7GCLNo ratings yet
- The Wild PartyDocument3 pagesThe Wild PartyMeganMcArthurNo ratings yet
- (Template) Grade 6 Science InvestigationDocument6 pages(Template) Grade 6 Science InvestigationYounis AhmedNo ratings yet
- Meta Trader 4Document2 pagesMeta Trader 4Alexis Chinchay AtaoNo ratings yet
- TAX & DUE PROCESSDocument2 pagesTAX & DUE PROCESSMayra MerczNo ratings yet
- 2010 Economics Syllabus For SHSDocument133 pages2010 Economics Syllabus For SHSfrimpongbenardghNo ratings yet
- Consent 1095 1107Document3 pagesConsent 1095 1107Pervil BolanteNo ratings yet
- MA CHAPTER 2 Zero Based BudgetingDocument2 pagesMA CHAPTER 2 Zero Based BudgetingMohd Zubair KhanNo ratings yet
- IJAKADI: A Stage Play About Spiritual WarfareDocument9 pagesIJAKADI: A Stage Play About Spiritual Warfareobiji marvelous ChibuzoNo ratings yet
- The Steriotypes: Cultural StereotypeDocument8 pagesThe Steriotypes: Cultural StereotypeRosbeyli Mazara ReyesNo ratings yet
- List of Parts For Diy Dremel CNC by Nikodem Bartnik: Part Name Quantity BanggoodDocument6 pagesList of Parts For Diy Dremel CNC by Nikodem Bartnik: Part Name Quantity Banggoodyogesh parmarNo ratings yet
- Topic 1 in 21st CneturyDocument8 pagesTopic 1 in 21st CneturyLuwisa RamosNo ratings yet
- Comal ISD ReportDocument26 pagesComal ISD ReportMariah MedinaNo ratings yet
- Italy VISA Annex 9 Application Form Gennaio 2016 FinaleDocument11 pagesItaly VISA Annex 9 Application Form Gennaio 2016 Finalesumit.raj.iiit5613No ratings yet
- 14 Jet Mykles - Heaven Sent 5 - GenesisDocument124 pages14 Jet Mykles - Heaven Sent 5 - Genesiskeikey2050% (2)
- Search Inside Yourself PDFDocument20 pagesSearch Inside Yourself PDFzeni modjo02No ratings yet
- Complicated Grief Treatment Instruction ManualDocument276 pagesComplicated Grief Treatment Instruction ManualFrancisco Matías Ponce Miranda100% (3)