You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Academic Progress ReportDocument5 pagesAcademic Progress ReportArmansyah maulana harahapNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Corruption of Journal Impact Factors: Anurag A. AgrawalDocument2 pagesCorruption of Journal Impact Factors: Anurag A. AgrawalArmansyah maulana harahapNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- 2018 CMB Graduate Hbid CareersDocument10 pages2018 CMB Graduate Hbid CareersArmansyah maulana harahapNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Guidance For Industry Estimating The Maximum Safe Starting Dose in Initial Clinical Trials For Therapeutics in Adult Healthy VolunteersDocument30 pagesGuidance For Industry Estimating The Maximum Safe Starting Dose in Initial Clinical Trials For Therapeutics in Adult Healthy Volunteersaji_koeandaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Bawean DeerDocument9 pagesBawean DeerArmansyah maulana harahapNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- OSMOREGULATION & EXCRETION IN MARINE ORGANISMSDocument10 pagesOSMOREGULATION & EXCRETION IN MARINE ORGANISMSArmansyah maulana harahapNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Mahasiswa Tugas RutinDocument24 pagesMahasiswa Tugas RutinArmansyah maulana harahapNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Mahasiswa Tugas RutinDocument24 pagesMahasiswa Tugas RutinArmansyah maulana harahapNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 10.2305 IUCN - UK.2016-1.RLTS.T17975A17966347.enDocument16 pages10.2305 IUCN - UK.2016-1.RLTS.T17975A17966347.enArmansyah maulana harahapNo ratings yet
- Fertilization: Beginning A New OrganismDocument5 pagesFertilization: Beginning A New OrganismArmansyah maulana harahapNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
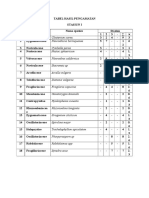
- Tabel Hasil PengamatanDocument1 pageTabel Hasil PengamatanArmansyah maulana harahapNo ratings yet
- Tabel Hasil PengamatanDocument1 pageTabel Hasil PengamatanArmansyah maulana harahapNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Pen ClingDocument6 pagesPen ClingArmansyah maulana harahapNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- No Family Spesies Juml Ah Pi LN Pi Pilnpi: Penium Spirostiolatum Tabelllaria Procculsa Gonatozygon KinahaniDocument5 pagesNo Family Spesies Juml Ah Pi LN Pi Pilnpi: Penium Spirostiolatum Tabelllaria Procculsa Gonatozygon KinahaniArmansyah maulana harahapNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Lupus: PrintDocument24 pagesLupus: Printmelodia gandezaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Nephrotic Syndrome in Children: The Indian Journal of Medical Research August 2005Document17 pagesNephrotic Syndrome in Children: The Indian Journal of Medical Research August 2005Hosne araNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Medications that may affect blood donation eligibilityDocument2 pagesMedications that may affect blood donation eligibilityNatasha MendozaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- KDIGO Transplantation GuidelinesDocument2 pagesKDIGO Transplantation GuidelinesSoteres VrachnesNo ratings yet
- Quiz Hematology Oncology Part 2 of 2Document60 pagesQuiz Hematology Oncology Part 2 of 2MedShare100% (5)
- Rovin 2019Document13 pagesRovin 2019hanzelNo ratings yet
- What Are Immunosuppressants?Document3 pagesWhat Are Immunosuppressants?ghifaryNo ratings yet
- 30926722: 2019 Update of The EULAR Recommendations For The Management of Systemic Lupus ErythematosusDocument10 pages30926722: 2019 Update of The EULAR Recommendations For The Management of Systemic Lupus ErythematosusLuis Enrique Caceres AlavrezNo ratings yet
- Treatment of Lupus Nephritis-1Document12 pagesTreatment of Lupus Nephritis-1Elizabeth MosqueraNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- KDIGO 2021 Glomerular Diseases GuidelineDocument276 pagesKDIGO 2021 Glomerular Diseases GuidelineAmbulatório Dieta Cetogênica HUBNo ratings yet
- Life Saving Medicine PDFDocument15 pagesLife Saving Medicine PDFInTan PermataNo ratings yet
- Harrison SLEDocument11 pagesHarrison SLEpazucenaNo ratings yet
- Mycophenolate MofetilDocument1 pageMycophenolate MofetilAndyPua100% (1)
- Risk Minimization Activity (ARMML)Document11 pagesRisk Minimization Activity (ARMML)Eman ShalabyNo ratings yet
- Module 5Document41 pagesModule 5Logical ThinkerNo ratings yet
- Liver TransplantsDocument6 pagesLiver Transplantssadaq84No ratings yet
- 18 Main CH21.docx 1Document46 pages18 Main CH21.docx 1Emily AnnNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Concord Biotech Ltd-IPO NoteDocument11 pagesConcord Biotech Ltd-IPO NoteSabyasachi JenaNo ratings yet
- Therapy of Diffuse or Focal Proliferative Lupus Nephritis - UpToDateDocument28 pagesTherapy of Diffuse or Focal Proliferative Lupus Nephritis - UpToDateJulio Camacho100% (1)
- Nephrology Fellow Clinical Compendium Kidney Transplant ChapterDocument21 pagesNephrology Fellow Clinical Compendium Kidney Transplant ChapterOsman fadilNo ratings yet
- KDIGO 2023 Lupus Nephritis Guideline - Public Review - 9 Mar 2023 PDFDocument102 pagesKDIGO 2023 Lupus Nephritis Guideline - Public Review - 9 Mar 2023 PDFlucasnatalia21bNo ratings yet
- FACTS: There Is No Cure & Complete: Sustained Remissions Are Rare. Principles of TherapyDocument12 pagesFACTS: There Is No Cure & Complete: Sustained Remissions Are Rare. Principles of TherapyAzizan HannyNo ratings yet
- Effects of Immunosuppressive Drugs On Platelet Aggregation and Soluble P Selectin Levels in Renal Transplant PatientsDocument8 pagesEffects of Immunosuppressive Drugs On Platelet Aggregation and Soluble P Selectin Levels in Renal Transplant PatientsNasiru BelloNo ratings yet
- Kidney TransplantDocument73 pagesKidney TransplantwatztanjaNo ratings yet
- MOH PAPER Prometric ExamDocument58 pagesMOH PAPER Prometric ExamRPh Farhatain100% (3)
- FSR Physicians Protocol1Document32 pagesFSR Physicians Protocol1Nishtha SinghalNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 10 Dec 2015 171411190GDI51SI2ProjectreportforpollutionDocument28 pages10 Dec 2015 171411190GDI51SI2ProjectreportforpollutionNajeeb HasanNo ratings yet
- Lupus NephritisDocument29 pagesLupus NephritisMuhammad Julpian0% (1)
- Perioperative Management GuidelineDocument10 pagesPerioperative Management Guidelineblue diamondNo ratings yet
- CCID 75908 Management of Pemphigus Vulgaris Challenges and Solutions 102115Document7 pagesCCID 75908 Management of Pemphigus Vulgaris Challenges and Solutions 102115M Marliando Satria PangestuNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)