You might also like
- Apley & Solomon's Fraktur ClaviculaDocument3 pagesApley & Solomon's Fraktur ClaviculaChiki CacaNo ratings yet
- C2 (Axis) FracturesDocument12 pagesC2 (Axis) FracturesSetyo Budi Premiaji WidodoNo ratings yet
- Pathology Mechanism: Jefferson Fracture Is The Eponymous Name Given To A Burst Fracture ofDocument25 pagesPathology Mechanism: Jefferson Fracture Is The Eponymous Name Given To A Burst Fracture ofAtikah FairuzNo ratings yet
- Fractures of The Cervical Spine: ReviewDocument7 pagesFractures of The Cervical Spine: ReviewMeri Fitria HandayaniNo ratings yet
- Acute Elbow Dislocations: Mechanisms, Classification, Associated InjuriesDocument7 pagesAcute Elbow Dislocations: Mechanisms, Classification, Associated Injuriesharpreet singhNo ratings yet
- Nirula Mayberry 2010 Article Commentary Rib Fracture Fixation Controversies and Technical ChallengesDocument10 pagesNirula Mayberry 2010 Article Commentary Rib Fracture Fixation Controversies and Technical ChallengesToàn NguyễnNo ratings yet
- Chapter 38 - Thoracic TraumaDocument24 pagesChapter 38 - Thoracic TraumaHamilton Delgado100% (1)
- Fracture in Leg Tibia and FibulaDocument27 pagesFracture in Leg Tibia and Fibulachilsya shajiNo ratings yet
- 11.clavicle Fractures REVDocument11 pages11.clavicle Fractures REVRika Yulizah GobelNo ratings yet
- The Knee - Breaking The MR ReflexDocument20 pagesThe Knee - Breaking The MR ReflexManiDeep ReddyNo ratings yet
- The Management of Flail Chest: Brian L. Pettiford, MD, James D. Luketich, MD, Rodney J. Landreneau, MDDocument9 pagesThe Management of Flail Chest: Brian L. Pettiford, MD, James D. Luketich, MD, Rodney J. Landreneau, MDVan Irish VentilacionNo ratings yet
- Calcaneal Fractures Where Are We NowDocument11 pagesCalcaneal Fractures Where Are We NowfunmugNo ratings yet
- Litrev SCHDocument7 pagesLitrev SCHdedyalkarni08No ratings yet
- Femoral Neck Fracture ImagingDocument13 pagesFemoral Neck Fracture ImagingRosemarie AbelaNo ratings yet
- Clavicle Fracture - TeachMeSurgeryDocument3 pagesClavicle Fracture - TeachMeSurgeryTeshanKoralageNo ratings yet
- Disorders of The Sternoclavicular Joint: SoulderDocument14 pagesDisorders of The Sternoclavicular Joint: SoulderFillipe AgraNo ratings yet
- Clavicle Fractures - StatPearls - NCBI BookshelfDocument9 pagesClavicle Fractures - StatPearls - NCBI BookshelfRizqan Fahlevvi AkbarNo ratings yet
- Muscle Injury of The Chest Wall and Upper ExtremityDocument10 pagesMuscle Injury of The Chest Wall and Upper Extremitylita34No ratings yet
- Jurnal RadiologyDocument3 pagesJurnal RadiologyStefania MarlinaNo ratings yet
- Chest RadiografphsDocument5 pagesChest RadiografphsMarijana KnezovicNo ratings yet
- Orbital TraumaDocument20 pagesOrbital TraumaJezreel Ortiz AscenciónNo ratings yet
- Treating Proximal Interphalangeal Joint Dislocations 2018Document10 pagesTreating Proximal Interphalangeal Joint Dislocations 2018royvillafrancaNo ratings yet
- Humerus FractureDocument5 pagesHumerus FracturecyahiminNo ratings yet
- Spine and Spinal Cord Injury Guide: Causes, Symptoms and TreatmentsDocument47 pagesSpine and Spinal Cord Injury Guide: Causes, Symptoms and TreatmentsAde Zulfiah100% (1)
- Anatomy of Spinal CordDocument43 pagesAnatomy of Spinal CordGargi MPNo ratings yet
- Fractures of Clavicle AserDocument44 pagesFractures of Clavicle AserHeba ElgoharyNo ratings yet
- Management of Mandibular Angle FractureDocument10 pagesManagement of Mandibular Angle FractureRudnapon AmornlaksananonNo ratings yet
- 76040138-Referat-Fraktur-Pelvis EditDocument34 pages76040138-Referat-Fraktur-Pelvis Editsri wulanNo ratings yet
- LBM 4 - Signs, Classification, Diagnosis and Complications of Pelvic FracturesDocument6 pagesLBM 4 - Signs, Classification, Diagnosis and Complications of Pelvic FracturesindahsariNo ratings yet
- The Unstable ElbowDocument17 pagesThe Unstable ElbowwerwrNo ratings yet
- Triangular Fibrocartilage Complex Lesions - A Classification (Palmer Classification)Document13 pagesTriangular Fibrocartilage Complex Lesions - A Classification (Palmer Classification)alobrienNo ratings yet
- Initial Management of Acute Spinal Cord Injury: Stephen Bonner MRCP FRCA FFICM Caroline Smith FRCADocument8 pagesInitial Management of Acute Spinal Cord Injury: Stephen Bonner MRCP FRCA FFICM Caroline Smith FRCAMinaz PatelNo ratings yet
- Literature ReviewsDocument16 pagesLiterature ReviewssyahmibestNo ratings yet
- Elbow DislocationDocument6 pagesElbow DislocationNadiatul HasanahNo ratings yet
- Frienchzel Joy A. Asis Group 3 BSN 3-ADocument14 pagesFrienchzel Joy A. Asis Group 3 BSN 3-AKenneth Louis GalizaNo ratings yet
- ORIF Radius and Ulna ProcedureDocument7 pagesORIF Radius and Ulna ProcedurealcojonicNo ratings yet
- Spinal Cord InjuryDocument91 pagesSpinal Cord InjuryPrabaningrum DwidjoasmoroNo ratings yet
- Blunt Chest TraumaDocument7 pagesBlunt Chest TraumaCatherine MorrisNo ratings yet
- Management of Shoulder DislocationsDocument9 pagesManagement of Shoulder Dislocationsamal.fathullahNo ratings yet
- Injuries of Shoulder Girdle Clavicle Fracture Scapula FractureDocument31 pagesInjuries of Shoulder Girdle Clavicle Fracture Scapula FractureWinda LiraNo ratings yet
- Arthroscopic Bankart RepairDocument14 pagesArthroscopic Bankart RepairDavid Paul RajNo ratings yet
- Imaging - Lecture 3 (Fractures)Document11 pagesImaging - Lecture 3 (Fractures)Adham MohamedNo ratings yet
- Bone Fractures - RadiologyDocument43 pagesBone Fractures - RadiologyMajd MustafaNo ratings yet
- Current Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiDocument8 pagesCurrent Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiJoão Artur BonadimanNo ratings yet
- 05 - Spinal Cord InjuryDocument92 pages05 - Spinal Cord InjurywaqarsuparcoNo ratings yet
- Shoulder ConditionsDocument8 pagesShoulder ConditionsCarlos GonzalesNo ratings yet
- Clavicula FractureDocument6 pagesClavicula Fracturedrian pamungkasNo ratings yet
- Orthopedic: Lec.11 DR - Hasan Abdulhadi.MDocument10 pagesOrthopedic: Lec.11 DR - Hasan Abdulhadi.MninaNo ratings yet
- Shoulder Injuries GuideDocument32 pagesShoulder Injuries Guidemontserrat santiago sanchezNo ratings yet
- Comminuted Patella FracturesDocument8 pagesComminuted Patella FracturesKirana lupitaNo ratings yet
- FxClavícula PDFDocument7 pagesFxClavícula PDFPenélope CrespoNo ratings yet
- Traumatic Injuries of The Diaphragm: Overview of Imaging Findings and DiagnosisDocument8 pagesTraumatic Injuries of The Diaphragm: Overview of Imaging Findings and DiagnosisWahyu IndraNo ratings yet
- Evaluation and Management of Acute Cervical Spine Trauma-RKY-finalDocument84 pagesEvaluation and Management of Acute Cervical Spine Trauma-RKY-finalRickky MDNo ratings yet
- Femoral Shaft FractureDocument5 pagesFemoral Shaft FracturePrimrose Gale ParingitNo ratings yet
- Basic Paediatrics - Unit 1 - SupracondylarDocument8 pagesBasic Paediatrics - Unit 1 - SupracondylarMohamad RamadanNo ratings yet
- Savetamal 2008Document10 pagesSavetamal 2008Eriekafebriayana RNo ratings yet
- Acromioclavicular InjuriesDocument11 pagesAcromioclavicular Injurieslou_gehrig2001No ratings yet
- Forearm and Wrist FracturesDocument34 pagesForearm and Wrist FracturesFatemeh DerakhshanNo ratings yet
- Acute Compartment Syndrome of The Upper Extremity: Review ArticleDocument17 pagesAcute Compartment Syndrome of The Upper Extremity: Review ArticleAskarNo ratings yet
- Neck Trauma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNeck Trauma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cancer Registry Peraboi Breast: Identitas PasienDocument2 pagesCancer Registry Peraboi Breast: Identitas PasienstevenNo ratings yet
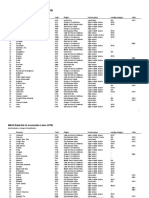
- World Bank list of economies by region and incomeDocument30 pagesWorld Bank list of economies by region and incomeSanjin Sanjke CattunarNo ratings yet
- Panitia Nasional Uji Kompetensi Mahasiswa Program Profesi DokterDocument127 pagesPanitia Nasional Uji Kompetensi Mahasiswa Program Profesi DokterNonaneneeNo ratings yet
- Central Venous Pressure (CVP)Document2 pagesCentral Venous Pressure (CVP)cado_arifNo ratings yet
- Ceklist Suhu FresserDocument2 pagesCeklist Suhu FresserstevenNo ratings yet
- Penatalaksanaan Ketoasidosis Diabetik (Kad)Document13 pagesPenatalaksanaan Ketoasidosis Diabetik (Kad)Emir AfifNo ratings yet
- Materi Bahasa Jepang Dasar IDocument6 pagesMateri Bahasa Jepang Dasar IstevenNo ratings yet
- AVM CnsDocument31 pagesAVM CnsGamma KnifeNo ratings yet
- Natural Hazards Congress 2018 12782 Abstract Template88520Document1 pageNatural Hazards Congress 2018 12782 Abstract Template88520MFaisalAbdaHasanNo ratings yet
- Spinal Cord DiseasesDocument14 pagesSpinal Cord DiseasesstevenNo ratings yet
- Guideline: Updates On Hiv and Infant FeedingDocument68 pagesGuideline: Updates On Hiv and Infant FeedingHerry SasukeNo ratings yet
- Review Articles Pathophysiology of Traumatic Brain Injury: C. Werner and K. EngelhardDocument6 pagesReview Articles Pathophysiology of Traumatic Brain Injury: C. Werner and K. EngelhardstevenNo ratings yet
- JNC 8 Guideline Algorithm for Treating HypertensionDocument2 pagesJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- Overview of Epidemiology: Rockwood & Green's Fractures in Adults, 6th EditionDocument53 pagesOverview of Epidemiology: Rockwood & Green's Fractures in Adults, 6th EditionSilvia TacheNo ratings yet
- Clavicle FractureDocument6 pagesClavicle FractureYbis LizarzaburuNo ratings yet
- Clavicle FractureDocument4 pagesClavicle FracturesridharNo ratings yet
- Jarvis 2017Document5 pagesJarvis 2017drelvNo ratings yet
- Master Techniques in Orthopaedic Surgery Fractures, 2nd Ed - Donal A. WissDocument1,766 pagesMaster Techniques in Orthopaedic Surgery Fractures, 2nd Ed - Donal A. WissCesar Adolfo Salamanca OntiverosNo ratings yet
- Fractures of The Upper LimbDocument3 pagesFractures of The Upper LimbJim Jose AntonyNo ratings yet
- Unstable Distal Clavicle Fractures (Neer Type II)Document21 pagesUnstable Distal Clavicle Fractures (Neer Type II)Orthopaedics & Trauma in YoutubeNo ratings yet
- Conservative Treatment of Clavicle FracturesDocument21 pagesConservative Treatment of Clavicle FracturesErwan Ahmad DNo ratings yet
- 3 5mmClavHookPlateDocument11 pages3 5mmClavHookPlatethomsoon01No ratings yet
- Blunt Chest TraumaDocument105 pagesBlunt Chest TraumasunliesNo ratings yet
- U01 Clavicle InjuriesDocument121 pagesU01 Clavicle Injuriesadrian_mogosNo ratings yet
- Aaos 2012Document190 pagesAaos 2012Yusufa ArdyNo ratings yet
- Clavicle FractureDocument15 pagesClavicle Fracturesalsabil aurellNo ratings yet
- Clavicle FractureDocument33 pagesClavicle FractureNitin AggarwalNo ratings yet
- Clavicle fracture classifications overviewDocument3 pagesClavicle fracture classifications overviewSachin MahajanNo ratings yet
- Clavicle Fracture Protocol After Surgical RepairDocument20 pagesClavicle Fracture Protocol After Surgical RepairNicoGeorgescuNo ratings yet
- Clavicle Fracture: Signs and SymptomsDocument4 pagesClavicle Fracture: Signs and SymptomsbvlbvlNo ratings yet
- Sports Injuries and Its PreventionDocument30 pagesSports Injuries and Its PreventionAkheel AhammedNo ratings yet
- Shoulder ConditionsDocument8 pagesShoulder ConditionsCarlos GonzalesNo ratings yet
- Nonunion of The Fractured ClavicleDocument18 pagesNonunion of The Fractured ClavicleJacobMsangNo ratings yet
- Clavicle Fracture Protocol Non SurgicalDocument17 pagesClavicle Fracture Protocol Non SurgicalAlbert MarcuNo ratings yet
- AC Plate On The Treatment of Fractures and Dislocation of Acromio-Clavicular Joint. J. Schmidt, A. WittDocument20 pagesAC Plate On The Treatment of Fractures and Dislocation of Acromio-Clavicular Joint. J. Schmidt, A. WittNuno Craveiro LopesNo ratings yet
- Sfa TechniquesDocument3 pagesSfa TechniquesSoriano ArmenioNo ratings yet
- Everything You Need to Know About Clavicle FracturesDocument41 pagesEverything You Need to Know About Clavicle FracturesHaidi SyuhairiNo ratings yet
- Clavicle FractureDocument121 pagesClavicle FractureMuhamad Agung SupriyantoNo ratings yet
- Orthopedics: Dr. C. Hutchison Kurt Droll and Christopher Gallimore, Editors Markku Nousiainen, Associate EditorDocument48 pagesOrthopedics: Dr. C. Hutchison Kurt Droll and Christopher Gallimore, Editors Markku Nousiainen, Associate Editordoterofthemosthigh100% (1)
- Clinical Upper Limb OsmosisDocument11 pagesClinical Upper Limb OsmosisAdirfah AmeriyaniNo ratings yet
- Clavicle FractureDocument17 pagesClavicle FractureM Caesar NovaldyNo ratings yet
- Fraktur KlavikulaDocument10 pagesFraktur KlavikulaEricsen T.P.No ratings yet
- Shoulder and Upper Extremity InjuriesDocument107 pagesShoulder and Upper Extremity InjuriesStaen KisNo ratings yet