You might also like
- Quality Assurance TechnicianDocument3 pagesQuality Assurance Technicianapi-77874686No ratings yet
- Postmortem Chemistry Update Part I: Review ArticleDocument12 pagesPostmortem Chemistry Update Part I: Review ArticleAna CruzNo ratings yet
- Instrument Required in Quality Control of Pharmaceutical IndustryDocument8 pagesInstrument Required in Quality Control of Pharmaceutical IndustrybharatheeeyuduNo ratings yet
- Sensory Evaluation in FoodDocument32 pagesSensory Evaluation in FoodAnonymous vVsidh3nNo ratings yet
- Standardization of Alcohol Calculations in ResearchDocument12 pagesStandardization of Alcohol Calculations in ResearchSava Vijak100% (1)
- Forensic ToxicologyDocument4 pagesForensic ToxicologyYusnida RahmawatiNo ratings yet
- D 4191 - 15Document4 pagesD 4191 - 15hydrogenperoksideNo ratings yet
- Determination of Benzoic Acid and Salicylic Acid PDFDocument5 pagesDetermination of Benzoic Acid and Salicylic Acid PDFFadilah QonitahNo ratings yet
- Estimation of Reducing Sugar by Nelson-Somogyi MethodDocument2 pagesEstimation of Reducing Sugar by Nelson-Somogyi Methodliska ramdanawati80% (5)
- EJMCM - Volume 9 - Issue 1 - Pages 526-531Document6 pagesEJMCM - Volume 9 - Issue 1 - Pages 526-531Faidzah Nuriyyah UlfahNo ratings yet
- Review of LiteratureDocument6 pagesReview of LiteratureAnonymous ekN8oq1mUNo ratings yet
- Aspectos Preanaliticos en Toxicologia PostmortemDocument26 pagesAspectos Preanaliticos en Toxicologia PostmortemDFNo ratings yet
- Laboratory Testing For Recent Alcohol Consumption: Comparison of Ethanol, Methanol, and 5-HydroxytryptopholDocument7 pagesLaboratory Testing For Recent Alcohol Consumption: Comparison of Ethanol, Methanol, and 5-HydroxytryptopholfranklyNo ratings yet
- A Case of Severe Hypertriglyceridaemia and HypercholesterolaemiaDocument1 pageA Case of Severe Hypertriglyceridaemia and Hypercholesterolaemiathys2000No ratings yet
- Sparrow 2012Document13 pagesSparrow 2012Elisa RodríguezNo ratings yet
- 2018 Alcohol Related Disease 15674Document28 pages2018 Alcohol Related Disease 15674Mihaela ShimanNo ratings yet
- Via de La ResacaDocument16 pagesVia de La ResacaDaniela Guerrero.No ratings yet
- Postmortem Biochemistry of Vitreous Humor and Glucose MetabolismDocument7 pagesPostmortem Biochemistry of Vitreous Humor and Glucose MetabolismsbeyeforhireNo ratings yet
- (Q1) Pone.0169593Document16 pages(Q1) Pone.0169593wiradewi lestariNo ratings yet
- Evaluation of Phosphatidylethanol by ELISA For Detection of Excessive Alcohol Use Compared With Traditional Biomarkers A Case Control StudyDocument7 pagesEvaluation of Phosphatidylethanol by ELISA For Detection of Excessive Alcohol Use Compared With Traditional Biomarkers A Case Control StudybrighteyezblueNo ratings yet
- Alcohol and Drugs in Epilepsy: Pathophysiology, Presentation, Possibilities, and PreventionDocument10 pagesAlcohol and Drugs in Epilepsy: Pathophysiology, Presentation, Possibilities, and PreventionAna Maria Gómez GonzálezNo ratings yet
- STAD211ECE B2 AlcoholAbuseDocument14 pagesSTAD211ECE B2 AlcoholAbuseAlfredo MorenoNo ratings yet
- (Q1) Pone.0169593Document16 pages(Q1) Pone.0169593wiradewi lestariNo ratings yet
- Labmed29 0102Document7 pagesLabmed29 0102MNo ratings yet
- Jurnal 10Document8 pagesJurnal 10Amelia Dwi Ramadhani AjitiaNo ratings yet
- Pharmacological and Pharmacokinetic Profile of The Novel Ocular Hypotensive Prodrug CKLP1 in Dutch-Belted Pigmented RabbitsDocument16 pagesPharmacological and Pharmacokinetic Profile of The Novel Ocular Hypotensive Prodrug CKLP1 in Dutch-Belted Pigmented RabbitsYayaaa aNo ratings yet
- (Alcoholism-Related Genetic Alteration) : Revista de Neurologia September 2003Document11 pages(Alcoholism-Related Genetic Alteration) : Revista de Neurologia September 2003andresoliverosgomezNo ratings yet
- Metabolic AcidosisDocument14 pagesMetabolic Acidosispara todoNo ratings yet
- Sepsis FrontierDocument14 pagesSepsis FrontierRafael Molina QuirozNo ratings yet
- Alteraciones Genéticas Relacionadas Con El Alcoholismo: M.D. EscarabajalDocument10 pagesAlteraciones Genéticas Relacionadas Con El Alcoholismo: M.D. EscarabajalFanny Marlene BiersackNo ratings yet
- Jurnal Alkohol KualitatifDocument8 pagesJurnal Alkohol KualitatifMastuti Widi LestariNo ratings yet
- The Impact of Delayed Analysis On Glucose Levels of Blood SamplesDocument4 pagesThe Impact of Delayed Analysis On Glucose Levels of Blood SamplesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cerebrospinal Fluid and Blood Biomarkers of Status Epilepticus - 2020Document40 pagesCerebrospinal Fluid and Blood Biomarkers of Status Epilepticus - 2020Reny Wane Vieira dos SantosNo ratings yet
- Assessment of Early Morning Serum Cortisol Levels in - 2022 - Medical Journal ADocument7 pagesAssessment of Early Morning Serum Cortisol Levels in - 2022 - Medical Journal AAnisha RanaNo ratings yet
- AlcoholDocument16 pagesAlcoholAna Maria BuenoNo ratings yet
- Hipertensión IntraabdominalDocument24 pagesHipertensión IntraabdominalAnonymous QNRRaQUNo ratings yet
- Abstracts CopenhagenDocument127 pagesAbstracts CopenhagenPisica ZmeuNo ratings yet
- Alcohol Addiction Research From Animal Models To ClinicsDocument12 pagesAlcohol Addiction Research From Animal Models To ClinicsJef_8No ratings yet
- Alcohol Calculations in Emergency and Forensic MedDocument7 pagesAlcohol Calculations in Emergency and Forensic MedSava VijakNo ratings yet
- Drug and Alcohol Dependence: Short CommunicationDocument5 pagesDrug and Alcohol Dependence: Short CommunicationAulas EspañolNo ratings yet
- PEth Concentrations Following Use of Hand SanitizerDocument12 pagesPEth Concentrations Following Use of Hand SanitizerbrighteyezblueNo ratings yet
- Cell Clot Vs PTS MetohdsDocument15 pagesCell Clot Vs PTS MetohdsAnil Chowadary Anil ChowadaryNo ratings yet
- Effects of Variation at The ALDH2 Locus On Alcohol Metabolism, Sensitivity, Consumption, and Dependence in EuropeansDocument8 pagesEffects of Variation at The ALDH2 Locus On Alcohol Metabolism, Sensitivity, Consumption, and Dependence in EuropeansamraovcinaNo ratings yet
- Pappolla Familial Hypercholesterolemia and Mild Cognitive ImpairmentDocument13 pagesPappolla Familial Hypercholesterolemia and Mild Cognitive ImpairmentMike Pappolla MD, PhDNo ratings yet
- Diabetic Post Mortem PDFDocument7 pagesDiabetic Post Mortem PDFPrakarsa Adi Daya NusantaraNo ratings yet
- Study of Serum Electrolytes in Acute Exacerbation of Chronic Obstructive Pulmonary Disease PatientsDocument4 pagesStudy of Serum Electrolytes in Acute Exacerbation of Chronic Obstructive Pulmonary Disease PatientsTri UtomoNo ratings yet
- Alcohol and CognitionDocument9 pagesAlcohol and CognitionKaren VelázquezNo ratings yet
- Panneerselvam2016 PDFDocument11 pagesPanneerselvam2016 PDFSabrina Umi KhabibahNo ratings yet
- Molecular Basis of AlcoholismDocument23 pagesMolecular Basis of AlcoholismVerónica RomeroNo ratings yet
- Jurnal 6 1 JuniDocument16 pagesJurnal 6 1 Junipencari pencerahan45No ratings yet
- Plasma Homocysteine and Total Thiol Content in Patients With Exudative Age-Related Macular DegenerationDocument5 pagesPlasma Homocysteine and Total Thiol Content in Patients With Exudative Age-Related Macular DegenerationAnonymous 1jCVqQuNo ratings yet
- Clinics in Laboratory MedicineDocument15 pagesClinics in Laboratory MedicineMárcio RodriguesNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument10 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaReuben JosephNo ratings yet
- Clinical Study: Serum Antioxidative Enzymes Levels and Oxidative Stress Products in Age-Related Cataract PatientsDocument7 pagesClinical Study: Serum Antioxidative Enzymes Levels and Oxidative Stress Products in Age-Related Cataract PatientsStrangersNo ratings yet
- Shefa 2017Document6 pagesShefa 2017chaak castellanosNo ratings yet
- Cakir2021 Lactatealbumin Ratio Is More Effective Than Lactate or Albumin Alone in Predicting Clinical Outcomes in Intensive Care Patients With SepsisDocument6 pagesCakir2021 Lactatealbumin Ratio Is More Effective Than Lactate or Albumin Alone in Predicting Clinical Outcomes in Intensive Care Patients With SepsisRazan RabiNo ratings yet
- Temporal Relationship Between Lens Protein Oxidation and Cataract Development in Streptozotocin-Induced Diabetic RatsDocument6 pagesTemporal Relationship Between Lens Protein Oxidation and Cataract Development in Streptozotocin-Induced Diabetic RatsFitri Nur DiniNo ratings yet
- Poisoning and The Pathologist: C H A P T E RDocument12 pagesPoisoning and The Pathologist: C H A P T E RTrans TourNo ratings yet
- IPEG Guidelines For The Recording and Evaluation of Pharmaco-EEG Data in ManDocument20 pagesIPEG Guidelines For The Recording and Evaluation of Pharmaco-EEG Data in Mansvetlavb8063No ratings yet
- A Case-Comparison Study of Executive Functions in Alcohol-Dependent Adults With Maternal History of AlcoholismDocument6 pagesA Case-Comparison Study of Executive Functions in Alcohol-Dependent Adults With Maternal History of AlcoholismmirymirelaNo ratings yet
- Pmls ArticleDocument8 pagesPmls ArticleEd dela PenaNo ratings yet
- J of Bone Mineral Res - 2022 - El Hajj Fuleihan - Classical and Nonclassical Manifestations of PrimaryDocument21 pagesJ of Bone Mineral Res - 2022 - El Hajj Fuleihan - Classical and Nonclassical Manifestations of Primarykobag87897No ratings yet
- Inositol Analysis HPLCDocument9 pagesInositol Analysis HPLCAnton MelcherNo ratings yet
- Nihms718761 PDFDocument9 pagesNihms718761 PDFAnton MelcherNo ratings yet
- Clinical Medical Reviews and Case Reports: ClinmedDocument6 pagesClinical Medical Reviews and Case Reports: ClinmedConciencia CristalinaNo ratings yet
- Jurnal Reading A Meta-Analysis of Antibiotics Versus Surgery For The Treatment of Acute AppendicitisDocument1 pageJurnal Reading A Meta-Analysis of Antibiotics Versus Surgery For The Treatment of Acute AppendicitisredityoNo ratings yet
- Tulipan 2018Document7 pagesTulipan 2018redityoNo ratings yet
- Morning ReportDocument8 pagesMorning ReportredityoNo ratings yet
- Leiomyoma of Vulva Mimmicking Bartholin Cyst: Anju Singh, Bharti Goel, Navneet Takkar, Ekta JainDocument3 pagesLeiomyoma of Vulva Mimmicking Bartholin Cyst: Anju Singh, Bharti Goel, Navneet Takkar, Ekta JainredityoNo ratings yet
- Clinical Pathology of Bartholin's Glands: A Review of The LiteratureDocument4 pagesClinical Pathology of Bartholin's Glands: A Review of The LiteratureredityoNo ratings yet
- AbdomenDocument37 pagesAbdomenredityoNo ratings yet
- 31306a9a.pdf: Obesity and Weight-Loss Medication. 2016:2 (1) :1-7Document1 page31306a9a.pdf: Obesity and Weight-Loss Medication. 2016:2 (1) :1-7redityoNo ratings yet
- Patologi Lingkungan: (Enviromental Disease)Document91 pagesPatologi Lingkungan: (Enviromental Disease)redityoNo ratings yet
- Article1379775512 - Oluyemi Et AlDocument3 pagesArticle1379775512 - Oluyemi Et AlredityoNo ratings yet
- BHIVA Audit ParticipantsDocument3 pagesBHIVA Audit ParticipantsredityoNo ratings yet
- Rheumatoid Arthritis: Herni Suprapti DR MkesDocument63 pagesRheumatoid Arthritis: Herni Suprapti DR MkesredityoNo ratings yet
- HP Lung Faal PBLDocument32 pagesHP Lung Faal PBLredityoNo ratings yet
- ParotitisDocument6 pagesParotitisredityoNo ratings yet
- (102163396) BiokimDocument13 pages(102163396) BiokimredityoNo ratings yet
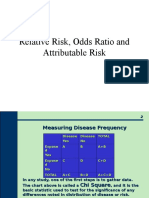
- Or RR PressentationDocument13 pagesOr RR PressentationredityoNo ratings yet
- Malaria Parasites Form Filamentous Cell-To-Cell Connections During Reproduction in The Mosquito MidgutDocument14 pagesMalaria Parasites Form Filamentous Cell-To-Cell Connections During Reproduction in The Mosquito MidgutredityoNo ratings yet
- Biochemical and Molecular Actions of NutrientsDocument5 pagesBiochemical and Molecular Actions of NutrientsredityoNo ratings yet
- SPECTROPHOTOMETER Practical Handout 2nd Year MBBSDocument7 pagesSPECTROPHOTOMETER Practical Handout 2nd Year MBBSIMDCBiochem100% (1)
- Experiment 2: Investigation Into The Kinetic Behaviour of Aqueous Crystal Violet SolutionsDocument15 pagesExperiment 2: Investigation Into The Kinetic Behaviour of Aqueous Crystal Violet SolutionsasdasNo ratings yet
- FORMULATION AND EVALUATION OF MICONAZOLE NITRATE LOADED NANOSPONGES FOR VAGINAL DRUG DELIVERY P.Suresh Kumar, N.Hematheerthani J.Vijaya Ratna and V.SaikishorDocument10 pagesFORMULATION AND EVALUATION OF MICONAZOLE NITRATE LOADED NANOSPONGES FOR VAGINAL DRUG DELIVERY P.Suresh Kumar, N.Hematheerthani J.Vijaya Ratna and V.SaikishoriajpsNo ratings yet
- Brochure Bsa3000 WebDocument4 pagesBrochure Bsa3000 WebDeni Ardian100% (1)
- Green Synthesis of Copper Nanoparticles and Its CharacterizationDocument5 pagesGreen Synthesis of Copper Nanoparticles and Its CharacterizationNicolas MolinaNo ratings yet
- Validation On Analysis Method For Phosphorus in Solid Inorganic Fertilizer Using UVvisible SpectrophotometryDocument10 pagesValidation On Analysis Method For Phosphorus in Solid Inorganic Fertilizer Using UVvisible SpectrophotometryBayu WiyantokoNo ratings yet
- Determination of Nickel As The Dimethylglyoxime Complex by SpectrophotometryDocument5 pagesDetermination of Nickel As The Dimethylglyoxime Complex by Spectrophotometryevenspase7859No ratings yet
- Analytical MethodsDocument165 pagesAnalytical MethodsMohamed MahgoubNo ratings yet
- Meat ScienceDocument9 pagesMeat ScienceIsworo RukmiNo ratings yet
- Alaya Sekar ISTFES 2023 RevisedDocument8 pagesAlaya Sekar ISTFES 2023 RevisedHunterz ScopeNo ratings yet
- Total Lipid Reagent Set (Colorimeyric Method) : Procedures (Manual)Document2 pagesTotal Lipid Reagent Set (Colorimeyric Method) : Procedures (Manual)Savrabh BhosaleNo ratings yet
- Shimadzu Spesification UV-1900Document1 pageShimadzu Spesification UV-1900Joy HendryNo ratings yet
- Optical Method of AnalysisDocument9 pagesOptical Method of AnalysisJohn Kevin San JoseNo ratings yet
- Quick Start Guide To Shimadzu UVDocument3 pagesQuick Start Guide To Shimadzu UVchemchemhaNo ratings yet
- Formulation Development and Evaluation of Self Nano Emulsifying Drug Delivery System of DolutegravirDocument15 pagesFormulation Development and Evaluation of Self Nano Emulsifying Drug Delivery System of DolutegravirEditor IJTSRDNo ratings yet
- SpectrophotometerDocument46 pagesSpectrophotometerSivakumar KNo ratings yet
- Exp No. 11 Chem Process Lab ReportDocument5 pagesExp No. 11 Chem Process Lab ReportSourav SutradharNo ratings yet
- BYK MacDocument5 pagesBYK MacNatdanai LimprasertNo ratings yet
- New Expt 8 Spectroscopy Lab Chlorophyll With SpectroVisDocument12 pagesNew Expt 8 Spectroscopy Lab Chlorophyll With SpectroVisAdam Bryant PoonawalaNo ratings yet
- 201 Thin-Layer Chromatographic Identification TestDocument2 pages201 Thin-Layer Chromatographic Identification TestCordinadores ControlNo ratings yet
- FAQ HP DesignJet Z6 and Z9+Document38 pagesFAQ HP DesignJet Z6 and Z9+tselcobklNo ratings yet
- 1 MODEL V-1100D Visible Spectrophotometer 1 Set 16.500.000 16.500.000 Single Beam Iso 9001, Ce Tuv GMBH Model V-1100D SpecificationDocument1 page1 MODEL V-1100D Visible Spectrophotometer 1 Set 16.500.000 16.500.000 Single Beam Iso 9001, Ce Tuv GMBH Model V-1100D Specificationeko nur wahyudiNo ratings yet
- Very Poor Poor Good Very Good Excellen TDocument11 pagesVery Poor Poor Good Very Good Excellen TNanthan DevNo ratings yet
- Certificate of Analysis Template For ChemicalDocument4 pagesCertificate of Analysis Template For ChemicalMon J. KamadNo ratings yet