You might also like
- NUR 446 Complex Care Assessment Sheet-1Document5 pagesNUR 446 Complex Care Assessment Sheet-1Tyler GoodmanNo ratings yet
- Approved Abbreviations For Use in Clinical Records and Letters PDFDocument10 pagesApproved Abbreviations For Use in Clinical Records and Letters PDFwhateverworkNo ratings yet
- It U Physician Assessment SheetDocument2 pagesIt U Physician Assessment SheetCarlos JorgeNo ratings yet
- Nursing Day Plan - ExcelDocument1 pageNursing Day Plan - ExceltennyrbNo ratings yet
- Borang Ambulans CallDocument2 pagesBorang Ambulans Callleo89azman100% (1)
- 12 Drugs Acting On The Cardiovascular SystemDocument7 pages12 Drugs Acting On The Cardiovascular SystemJAN CAMILLE LENONNo ratings yet
- Neuro PerformaDocument5 pagesNeuro PerformaSara KhanNo ratings yet
- Pre-Hospital Assessment Sheet: Triage ScoreDocument2 pagesPre-Hospital Assessment Sheet: Triage Scoreratna purwitasariNo ratings yet
- High Risk Consent For PCIDocument1 pageHigh Risk Consent For PCISree Sowjanya PatibandlaNo ratings yet
- RECOVER Initiative CPR Reporting Sheet 2020. v3.2Document2 pagesRECOVER Initiative CPR Reporting Sheet 2020. v3.2Mohana Preethi MNo ratings yet
- Cot 2012 English Canada v02.02 1 0Document410 pagesCot 2012 English Canada v02.02 1 0MDBNo ratings yet
- Medical AbbreviationsDocument13 pagesMedical AbbreviationsMuhammed NajibNo ratings yet
- Preop+++Goal Anaesthesia Record FormsDocument5 pagesPreop+++Goal Anaesthesia Record FormsShimelis AssefaNo ratings yet
- Respiratory Examination - DR - Hammouri's Style: Rahaf Wardeh Internal Medicine 2016-2017Document5 pagesRespiratory Examination - DR - Hammouri's Style: Rahaf Wardeh Internal Medicine 2016-2017asdddNo ratings yet
- Pre-op Evaluation SummaryDocument1 pagePre-op Evaluation Summarysabbo morsNo ratings yet
- Quality Corner - Major TraumaDocument3 pagesQuality Corner - Major TraumaNorth Country EMSNo ratings yet
- Isbi Practice Guidelines For Burn Care Part 2 2018 PDFDocument90 pagesIsbi Practice Guidelines For Burn Care Part 2 2018 PDFAstri SuyataNo ratings yet
- Diagnosis of ShockDocument9 pagesDiagnosis of ShockRejina RavindranNo ratings yet
- Neurological Assessment FormDocument6 pagesNeurological Assessment FormM.A. Ch.No ratings yet
- Integrated ChecklistDocument2 pagesIntegrated ChecklistKena BenNo ratings yet
- Heparin Infusion Guideline PDFDocument3 pagesHeparin Infusion Guideline PDFbrigde_xNo ratings yet
- West Visayas State University: Nursing ProcessDocument4 pagesWest Visayas State University: Nursing ProcessPhylum Chordata100% (1)
- Intake and Output ChartDocument2 pagesIntake and Output ChartViral Chann3LNo ratings yet
- Supportive Supervision ChecklistDocument3 pagesSupportive Supervision Checklistgeorgeloto12100% (1)
- Nervous SystemDocument21 pagesNervous SystemZaara ChishtiNo ratings yet
- Ultimate ChecklstDocument1 pageUltimate ChecklstMark ObiasNo ratings yet
- Chest Pain System - DisorderDocument1 pageChest Pain System - DisorderAA DDNo ratings yet
- Cardiac Stent PriceDocument4 pagesCardiac Stent PriceMahmudul Hasan TusharNo ratings yet
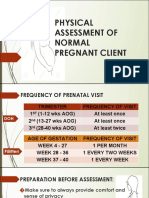
- Physical Assessment of a Pregnant ClientDocument25 pagesPhysical Assessment of a Pregnant ClientDe Leon, Austine Sydney D.No ratings yet
- Case Log TotalsDocument6 pagesCase Log Totalsnatalie nodayNo ratings yet
- Anaesthesia For LapDocument91 pagesAnaesthesia For LapAbhyuday KumarNo ratings yet
- Pediatric Emergency Pocket GuideDocument2 pagesPediatric Emergency Pocket GuideHongMingNo ratings yet
- Cot 2012Document410 pagesCot 2012AnonymousNo ratings yet
- Physician's Examination FormDocument1 pagePhysician's Examination FormMason FrasherNo ratings yet
- Nursing Assessment ToolDocument6 pagesNursing Assessment ToolRaniNo ratings yet
- Transthoracic Echocardiography Report: Reason For ExamDocument4 pagesTransthoracic Echocardiography Report: Reason For ExamJeff BakerNo ratings yet
- Corrected ElectrolytesDocument2 pagesCorrected Electrolytesdragon66100% (1)
- Principals of Paediatric History Taking and Physical ExaminationDocument17 pagesPrincipals of Paediatric History Taking and Physical ExaminationKingston HoNo ratings yet
- Issue 26 - The Nurse Advocate - Hamad Medical Corporation - July 2016Document20 pagesIssue 26 - The Nurse Advocate - Hamad Medical Corporation - July 2016Brent ForemanNo ratings yet
- ON-CALL ISSUES RESOLVEDDocument55 pagesON-CALL ISSUES RESOLVEDlatifaNo ratings yet
- Clinical Examination in Neonates: Yurita Handoyo DR., SpaDocument60 pagesClinical Examination in Neonates: Yurita Handoyo DR., SpaFebri ChristallagoNo ratings yet
- Med Cards AsprinDocument13 pagesMed Cards AsprinaliNo ratings yet
- Pre Medical Evaluatiom Form PFT 1 PDFDocument2 pagesPre Medical Evaluatiom Form PFT 1 PDFAIEN WENDELEIH Q. CAPINPIN100% (1)
- Neurological Examination PDFDocument6 pagesNeurological Examination PDFArif K BashaNo ratings yet
- Defibrillatorppt 131028115457 Phpapp01Document41 pagesDefibrillatorppt 131028115457 Phpapp01Simon JosanNo ratings yet
- Comprehensive Adult Health HistoryDocument7 pagesComprehensive Adult Health HistoryKhirsna PasajolNo ratings yet
- Packages Including Procedures, Rates and Minimum Documents Protocols and Other Details For New Phase of AB-MGRSBYDocument536 pagesPackages Including Procedures, Rates and Minimum Documents Protocols and Other Details For New Phase of AB-MGRSBYrudrasaaNo ratings yet
- Pediatrics (General Admissions) 5Document63 pagesPediatrics (General Admissions) 5Stanley ShanNo ratings yet
- Icu Adult and PaedsDocument2 pagesIcu Adult and PaedsPrashin RocharamNo ratings yet
- Half LifeDocument43 pagesHalf LifeMinal Nadeem100% (1)
- Critical Cardiac NotesDocument71 pagesCritical Cardiac NotesJamesNo ratings yet
- Bioinstrumentation II: Lecture 4: ECG MachineDocument30 pagesBioinstrumentation II: Lecture 4: ECG MachineHundessa DabaNo ratings yet
- Orders To Flush Central/hep Loc line/PICC: Admission D/CDocument2 pagesOrders To Flush Central/hep Loc line/PICC: Admission D/CKaren Joy DelayNo ratings yet
- HTTPS://WWW - Tvsmotor.com/iqube?utm Source Quora&utm Medium Paid&utm Campaign Quora Postlaunch Pratical ECDocument21 pagesHTTPS://WWW - Tvsmotor.com/iqube?utm Source Quora&utm Medium Paid&utm Campaign Quora Postlaunch Pratical ECAjithNo ratings yet
- Health: No Known AllergiesDocument12 pagesHealth: No Known AllergiesSeanmarie CabralesNo ratings yet
- Medical SignsDocument16 pagesMedical SignsOluwatobi FaniyiNo ratings yet
- MD001 - Medical Examinations Supplement - CurrentDocument3 pagesMD001 - Medical Examinations Supplement - CurrentNatalie DouglasNo ratings yet
- Anatomy RespDocument57 pagesAnatomy RespGunawan SamosirNo ratings yet
- AbbreviationDocument19 pagesAbbreviationJayson NatividadNo ratings yet
- Patient's Follow Up Profile SU1Document2 pagesPatient's Follow Up Profile SU1Faisol KabirNo ratings yet
- List of Fees For Consular Services and Other Matters As of 1 January 2019Document2 pagesList of Fees For Consular Services and Other Matters As of 1 January 2019Wilda AwliaNo ratings yet
- Guideline Hypoglycemia PDFDocument13 pagesGuideline Hypoglycemia PDFleslyjanet100% (1)
- Emergency Acls Reference Guide: Ecg Rhythm Examples and Aha Acls 2015 AlgorithmsDocument11 pagesEmergency Acls Reference Guide: Ecg Rhythm Examples and Aha Acls 2015 AlgorithmsWilda AwliaNo ratings yet
- Naso Orogastric Tube Management Guidelines For The Newborn V2.0 Sept 16 PDFDocument20 pagesNaso Orogastric Tube Management Guidelines For The Newborn V2.0 Sept 16 PDFWilda Awlia100% (1)
- Developmental CareDocument7 pagesDevelopmental CareWilda AwliaNo ratings yet
- The Newborn Early Warning (NEW) System: Development of An At-Risk Infant Intervention SystemDocument5 pagesThe Newborn Early Warning (NEW) System: Development of An At-Risk Infant Intervention Systemeneng latipa dewi100% (1)
- Bfhi Poster A2Document1 pageBfhi Poster A2api-423864945No ratings yet
- Emergency Acls Reference Guide: Ecg Rhythm Examples and Aha Acls 2015 AlgorithmsDocument11 pagesEmergency Acls Reference Guide: Ecg Rhythm Examples and Aha Acls 2015 AlgorithmsWilda AwliaNo ratings yet
- Examination of The Newborn InfantDocument15 pagesExamination of The Newborn InfantWilda AwliaNo ratings yet
- F E T C: Luid AND Lectrolyte Herapy IN HildrenDocument12 pagesF E T C: Luid AND Lectrolyte Herapy IN HildrenHartantoRezaGazaliNo ratings yet
- Gravity Feeding Drip Rate Chart: Home Care ServicesDocument2 pagesGravity Feeding Drip Rate Chart: Home Care ServicesWilda AwliaNo ratings yet
- Sample Application To DOHDocument1 pageSample Application To DOHWilda AwliaNo ratings yet
- Abdominal Wall DefectDocument10 pagesAbdominal Wall DefectWilda AwliaNo ratings yet
- Gravity Administration: This Is A Gravity Bag - Please Use This If The Pump FailsDocument2 pagesGravity Administration: This Is A Gravity Bag - Please Use This If The Pump FailsWilda AwliaNo ratings yet
- 0 - Speech & Debate WritingDocument12 pages0 - Speech & Debate WritingRituja DasNo ratings yet
- Zayd Tanbour - Final Draft of Research OutlineDocument2 pagesZayd Tanbour - Final Draft of Research Outlineapi-498084317No ratings yet
- Milk Handling PracticesDocument12 pagesMilk Handling Practicesbizuayehu admasuNo ratings yet
- Maimonides Medical Center - 2021-2022Document1 pageMaimonides Medical Center - 2021-2022sal palNo ratings yet
- Herbal Medicine in The Treatment of Patients With Type 2Document8 pagesHerbal Medicine in The Treatment of Patients With Type 2Abdul Laura CondulaNo ratings yet
- 5 Arrazi 34-42Document9 pages5 Arrazi 34-42NisaaNo ratings yet
- Nurs 05: Community Health Nursing 1 Community Health Nursing of Individual and Family As ClientDocument23 pagesNurs 05: Community Health Nursing 1 Community Health Nursing of Individual and Family As ClientToyour EternityNo ratings yet
- Accounting Information Systems 5th Edition Parkes Solutions ManualDocument36 pagesAccounting Information Systems 5th Edition Parkes Solutions Manualnubilegoggler.i8cm100% (14)
- Learning Environment Impacts StudentsDocument13 pagesLearning Environment Impacts Studentslourdes angeline barcomaNo ratings yet
- UntitledDocument478 pagesUntitledGghhNo ratings yet
- Inspiring Leaders April 2023Document54 pagesInspiring Leaders April 2023Jay MenonNo ratings yet
- BING Covid-19Document9 pagesBING Covid-19tirsha tjowasiNo ratings yet
- Hipoglikemi Diagnosa Dan TalakDocument19 pagesHipoglikemi Diagnosa Dan TalakPediatri 78 UndipNo ratings yet
- Red Cross Psychological First Aid BookDocument28 pagesRed Cross Psychological First Aid BookQuique ParadaNo ratings yet
- Characteristics of IODocument5 pagesCharacteristics of IOLynzae100% (2)
- Cmimorja e Produkteve Te HerbalifeDocument1 pageCmimorja e Produkteve Te HerbalifeDonat LikaNo ratings yet
- Psyc 311Document20 pagesPsyc 311laralesch2002No ratings yet
- Elc590: English For Oral Presentations: Resource Materials 3: Monroe's Motivated SequenceDocument22 pagesElc590: English For Oral Presentations: Resource Materials 3: Monroe's Motivated Sequencesarah adrianaNo ratings yet
- Spencer A. Rathus, Jeffrey S. Nevid, Lois Fichner-Rathus - Human Sexuality in A World of Diversity-Pearson Education (2014) PDFDocument677 pagesSpencer A. Rathus, Jeffrey S. Nevid, Lois Fichner-Rathus - Human Sexuality in A World of Diversity-Pearson Education (2014) PDFvric948100% (3)
- ACE Sports Nutrition For Health Professionals PagesDocument4 pagesACE Sports Nutrition For Health Professionals PagesHamada MansourNo ratings yet
- October JournalDocument36 pagesOctober Journalrammvr05No ratings yet
- Extraction of Caffeine From Tea Leaves Experiment Formal ReportDocument6 pagesExtraction of Caffeine From Tea Leaves Experiment Formal ReportChristeline Fernandez50% (2)
- Schizo Ppt.Document78 pagesSchizo Ppt.Nimisha ChackoNo ratings yet
- Analisis Jurnal Keperawatan HivDocument2 pagesAnalisis Jurnal Keperawatan HivMuhammad Khairul ZedNo ratings yet
- Guias Hta CKD 2023Document33 pagesGuias Hta CKD 2023miguel contrerasNo ratings yet
- Service Quality Study ReportDocument6 pagesService Quality Study ReportNIKHIL SINHANo ratings yet
- Haya 2 Semester 7Document3 pagesHaya 2 Semester 7api-317201750No ratings yet
- 276 Jaipal Singh VishwakarmaDocument8 pages276 Jaipal Singh Vishwakarmashubh1511No ratings yet
- Essential Intrapartum and Newborn CareDocument25 pagesEssential Intrapartum and Newborn CareMaria Lovelyn LumaynoNo ratings yet
- Assignment Ni Ayang Sa TechnologyDocument2 pagesAssignment Ni Ayang Sa TechnologyJohn Mico MacatigbacNo ratings yet