You might also like
- Social Security / Medicare Handbook for Federal Employees and Retirees: All-New 4th EditionFrom EverandSocial Security / Medicare Handbook for Federal Employees and Retirees: All-New 4th EditionNo ratings yet
- Assurant Health Access: in Force Underwriting Change PacketDocument10 pagesAssurant Health Access: in Force Underwriting Change PacketSwisskelly1No ratings yet
- 2023 - Oe - Notice - 2008 - FinalDocument5 pages2023 - Oe - Notice - 2008 - FinalabroughearNo ratings yet
- Patient Information Sheet 091409Document2 pagesPatient Information Sheet 091409api-16816262No ratings yet
- File Health Claim Form Blue Cross PlanDocument1 pageFile Health Claim Form Blue Cross PlanManoj GuptaNo ratings yet
- f10 Claim FormDocument2 pagesf10 Claim Formiceslurpie100% (1)
- JF Elite Plus Student Insurance Claim Form: ImportantDocument2 pagesJF Elite Plus Student Insurance Claim Form: ImportantJayesh GoplaniNo ratings yet
- School Employees Benefits Board (SEBB) Program Plan Overview and Cost of CoverageDocument4 pagesSchool Employees Benefits Board (SEBB) Program Plan Overview and Cost of CoverageRaisul ShakilNo ratings yet
- Marsh PNG Medicare CLAIM FORMDocument3 pagesMarsh PNG Medicare CLAIM FORMKaitaMahn100% (1)
- New Patient Forms 2018Document8 pagesNew Patient Forms 2018Rexy LasutNo ratings yet
- OVHC Claim Form 102017 PDFDocument3 pagesOVHC Claim Form 102017 PDFtarmudiNo ratings yet
- Doctor Statement Ssa 787Document3 pagesDoctor Statement Ssa 787Richard GuthNo ratings yet
- Saral Suraksha Bima, Plan - Preposal Form - v1Document3 pagesSaral Suraksha Bima, Plan - Preposal Form - v1rajeshNo ratings yet
- Waiver Form 2010 FallDocument2 pagesWaiver Form 2010 Fallmyself_pslNo ratings yet
- Patient Registration Packet 08/10Document5 pagesPatient Registration Packet 08/10Heart of the Valley, Pediatric CardiologyNo ratings yet
- FS PrivateInsuranceDocument2 pagesFS PrivateInsuranceIndiana Family to FamilyNo ratings yet
- Male New Patient Paperwork 5.2015Document8 pagesMale New Patient Paperwork 5.2015Muhammad AdeelNo ratings yet
- LTC Renewal PDFDocument12 pagesLTC Renewal PDFVashisth SoniNo ratings yet
- UIICHdfc ClaimformDocument2 pagesUIICHdfc ClaimformdomyomglolNo ratings yet
- Star Health Insurance Proposal FormDocument2 pagesStar Health Insurance Proposal FormBhaktha SinghNo ratings yet
- BLTD 8711054 Ae 3 de 58 eDocument3 pagesBLTD 8711054 Ae 3 de 58 eMahi RajputNo ratings yet
- Crewsure Claim Form (XLCatlin) 1.3Document2 pagesCrewsure Claim Form (XLCatlin) 1.3Andrei Belehuzi0% (1)
- All Savers - EE Enrollment FormDocument4 pagesAll Savers - EE Enrollment FormJohn PaulNo ratings yet
- Claim Health Care Benefits 19132ADocument2 pagesClaim Health Care Benefits 19132ACharles MoncyNo ratings yet
- Texas Employees Group Benefits Program (GBP) Supplemental Information Form For EmployeesDocument2 pagesTexas Employees Group Benefits Program (GBP) Supplemental Information Form For EmployeesBhargav Teja NukalaNo ratings yet
- Claimant Statement With ETF Mandate FormDocument6 pagesClaimant Statement With ETF Mandate FormKishan GarhtiyaNo ratings yet
- Claim Dental Care Expenses 19110ADocument2 pagesClaim Dental Care Expenses 19110Alizita777No ratings yet
- Supplementary Health Benefits Claim Form: Drug ExpensesDocument2 pagesSupplementary Health Benefits Claim Form: Drug ExpensesKaitlinMSNo ratings yet
- Application For Membership Form: Application No.: Effectivity Date: Contract No.Document2 pagesApplication For Membership Form: Application No.: Effectivity Date: Contract No.Lizeth QuerubinNo ratings yet
- Parivar Proposal FormDocument10 pagesParivar Proposal FormHANSDA DHIRENDRANATHANNo ratings yet
- Bundle 2012053110483376037Document7 pagesBundle 2012053110483376037ryanwoNo ratings yet
- Claim FormDocument4 pagesClaim Formmuhammad haroonNo ratings yet
- Dental and Vision Enrollment FormDocument3 pagesDental and Vision Enrollment Formsatnam_25No ratings yet
- Logo New Patient Packet 2016Document4 pagesLogo New Patient Packet 2016api-283388825No ratings yet
- Medical Release Form 27 PDFDocument2 pagesMedical Release Form 27 PDFDina Dwi RamadhaniNo ratings yet
- Your Dependent Child's Coverage May End SoonDocument3 pagesYour Dependent Child's Coverage May End Soonbigblockz8No ratings yet
- General Claim Submission Form: Section 1 - Plan Member InformationDocument2 pagesGeneral Claim Submission Form: Section 1 - Plan Member InformationRachelMayNo ratings yet
- f9 Refund Form OSHCDocument2 pagesf9 Refund Form OSHCSusi RamadhaniNo ratings yet
- NSTUMP - Proposal FormDocument7 pagesNSTUMP - Proposal FormJagadeesh MaheshNo ratings yet
- Shadowing/observation Application: Email Application To: or Fax: 417-269-4787Document5 pagesShadowing/observation Application: Email Application To: or Fax: 417-269-4787Bhumsen ThapaNo ratings yet
- Employee Enrollment Application: Group Size 51+ Eligible Employees - Medically UnderwrittenDocument6 pagesEmployee Enrollment Application: Group Size 51+ Eligible Employees - Medically Underwrittenmdugan5026No ratings yet
- GMHP Claim Form - Online PDFDocument4 pagesGMHP Claim Form - Online PDFSalem AmraneNo ratings yet
- Correspondence SBALTAZARDocument11 pagesCorrespondence SBALTAZARsandral.baltazar17No ratings yet
- STD Claim FormDocument8 pagesSTD Claim Formapi-314323052No ratings yet
- Cooperative Health Enrollment FormDocument2 pagesCooperative Health Enrollment FormGeraldine Daquipil TortalNo ratings yet
- Form 300Document8 pagesForm 300Sachin SharmaNo ratings yet
- Important:: CIGNA Group InsuranceDocument2 pagesImportant:: CIGNA Group InsuranceLoganBohannonNo ratings yet
- Gmail - Your Amerigroup Application - Important Plan InformationDocument2 pagesGmail - Your Amerigroup Application - Important Plan InformationIsmael LanderosNo ratings yet
- Sun Life FormDocument2 pagesSun Life FormGerald DicenNo ratings yet
- Proposal Form Ashakiran PDFDocument6 pagesProposal Form Ashakiran PDFSreejith Rajendran PillaiNo ratings yet
- Cigna TTK Lifestyle Protection Group Policy - Health InsuranceDocument4 pagesCigna TTK Lifestyle Protection Group Policy - Health InsuranceChrissy CattonNo ratings yet
- Anthem Blue Cross Medical Enrollment Form 2014Document4 pagesAnthem Blue Cross Medical Enrollment Form 2014Tanveer ShaikhNo ratings yet
- NTUC Claim FormDocument5 pagesNTUC Claim FormHihiNo ratings yet
- OMA OM en Claims TravelDelayDocument4 pagesOMA OM en Claims TravelDelayreshwan aliNo ratings yet
- Claim FormDocument3 pagesClaim FormInvestor ProtegeNo ratings yet
- 2011 2012 Spring Student - and - Dependent Installment EnrollmentDocument2 pages2011 2012 Spring Student - and - Dependent Installment Enrollmentdiana_siegel_3No ratings yet
- Time Away From Work Service Center InstructionsDocument17 pagesTime Away From Work Service Center InstructionsAlayssia CanoraNo ratings yet
- Your 2024 Social Security Cost of Living IncreaseDocument4 pagesYour 2024 Social Security Cost of Living IncreasenazoyaqNo ratings yet
- Hatfield Plaza - AB - Combined Floor Plan - Area A - TEMPLATEDocument1 pageHatfield Plaza - AB - Combined Floor Plan - Area A - TEMPLATEAndres Cedeno TutivenNo ratings yet
- Dipanel Galvalume PDFDocument1 pageDipanel Galvalume PDFAndres Cedeno TutivenNo ratings yet
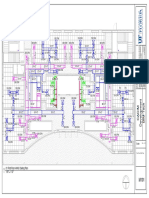
- Structural Sample DrawingDocument1 pageStructural Sample DrawingAndres Cedeno TutivenNo ratings yet
- Second Floor PlanDocument1 pageSecond Floor PlanAndres Cedeno TutivenNo ratings yet
- Dipanel Galvalume PDFDocument1 pageDipanel Galvalume PDFAndres Cedeno TutivenNo ratings yet
- BEXEL Manager-Getting StartedDocument11 pagesBEXEL Manager-Getting StartedAndres Cedeno TutivenNo ratings yet
- House PhotosDocument16 pagesHouse PhotosAndres Cedeno TutivenNo ratings yet
- Framing Work Block Done - Rev CDocument3 pagesFraming Work Block Done - Rev CAndres Cedeno TutivenNo ratings yet
- BIM NamingDocument8 pagesBIM NamingAndres Cedeno TutivenNo ratings yet
- 1/8" 1'-0" 1 01 First Floor HVAC Ceiling PlanDocument10 pages1/8" 1'-0" 1 01 First Floor HVAC Ceiling PlanAndres Cedeno TutivenNo ratings yet
- Building ModelsDocument1 pageBuilding ModelsAndres Cedeno TutivenNo ratings yet
- Cedeno - Assignment - L10 - Sheet - A103 - East and West ElevationsDocument1 pageCedeno - Assignment - L10 - Sheet - A103 - East and West ElevationsAndres Cedeno TutivenNo ratings yet
- Window Door SchedulesDocument1 pageWindow Door SchedulesAndres Cedeno TutivenNo ratings yet
- 1976 - House Technical Drawings PDFDocument5 pages1976 - House Technical Drawings PDFAndres Cedeno TutivenNo ratings yet
- CI1697-R - Bridge Modeling Approaches HandoutDocument22 pagesCI1697-R - Bridge Modeling Approaches HandoutAndres Cedeno TutivenNo ratings yet
- Document E202 - 2008: Building Information Modeling Protocol ExhibitDocument9 pagesDocument E202 - 2008: Building Information Modeling Protocol ExhibitAndres Cedeno TutivenNo ratings yet
- 05 Positive Vs Negative Iteration in DesignDocument12 pages05 Positive Vs Negative Iteration in DesignMelvin MolinaNo ratings yet
- Cedeno - Final Model LogDocument5 pagesCedeno - Final Model LogAndres Cedeno TutivenNo ratings yet
- Aiming For Continuous Flow: LCI White Paper-3 March 5, 1999 Glenn Ballard and Iris Tommelein, LCIDocument6 pagesAiming For Continuous Flow: LCI White Paper-3 March 5, 1999 Glenn Ballard and Iris Tommelein, LCIAndres Cedeno TutivenNo ratings yet
- Lean Project Delivery SystemDocument7 pagesLean Project Delivery SystemSebastian BernalNo ratings yet
- Concept DrawingsDocument4 pagesConcept DrawingsAndres Cedeno TutivenNo ratings yet
- Research AssignmentDocument3 pagesResearch AssignmentAndres Cedeno TutivenNo ratings yet
- LCI Glossary01152014 PDFDocument7 pagesLCI Glossary01152014 PDFAndres Cedeno TutivenNo ratings yet
- Koskela-Application of The New Production Philosophy To CosntructionDocument81 pagesKoskela-Application of The New Production Philosophy To CosntructionlmonteroNo ratings yet
- Applying Lean Construction To Loss Control: Xavier BriosoDocument11 pagesApplying Lean Construction To Loss Control: Xavier BriosoLuis Fernando Cruzalegui BonillaNo ratings yet
- Last Planner SystemDocument192 pagesLast Planner SystemJose Stein GuerreroNo ratings yet
- Last Planner SystemDocument192 pagesLast Planner SystemJose Stein GuerreroNo ratings yet
- Introduction To Project Planning - Bus Stop Case StudyDocument28 pagesIntroduction To Project Planning - Bus Stop Case StudyAndres Cedeno TutivenNo ratings yet
- Research AssignmentDocument3 pagesResearch AssignmentAndres Cedeno TutivenNo ratings yet
- EBS ConfigurationDocument11 pagesEBS ConfigurationLavanya Basa100% (1)
- CQC John Radcliffe ReportDocument99 pagesCQC John Radcliffe ReportOxfordMailEditorialNo ratings yet
- Bank Statement 2015 AugDocument4 pagesBank Statement 2015 AugKaykay HendersonNo ratings yet
- Banking Project: Name-Sanika Patil Class - Fybcom Div-B ROLL NO - 216Document15 pagesBanking Project: Name-Sanika Patil Class - Fybcom Div-B ROLL NO - 216sanika patilNo ratings yet
- Frederick's Account StatementDocument3 pagesFrederick's Account StatementArdan DiazNo ratings yet
- InvoiceDocument1 pageInvoicearcbyecommerceNo ratings yet
- Motorcycle Parts Inventory Management System: AbstractDocument8 pagesMotorcycle Parts Inventory Management System: AbstractFayyaz Gulammuhammad100% (1)
- Personal Bond Refund FormDocument2 pagesPersonal Bond Refund FormbestniazNo ratings yet
- NCHS President and CEO, Irma Cota, Announces RetirementDocument3 pagesNCHS President and CEO, Irma Cota, Announces RetirementPR.comNo ratings yet
- Lab Activity 1Document8 pagesLab Activity 1joyce KimNo ratings yet
- ACCA F2 Sample Study NoteDocument21 pagesACCA F2 Sample Study Notebillyryan10% (1)
- Introduction of Leadership (OSIM)Document7 pagesIntroduction of Leadership (OSIM)Azhar PropertyNo ratings yet
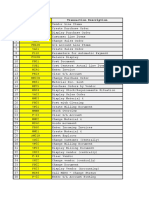
- SAP Transaction Code ModulesDocument6 pagesSAP Transaction Code ModulesVivek Shashikant SonawaneNo ratings yet
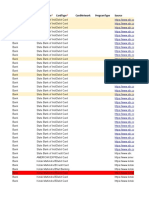
- List of service fees with dates and reference numbersDocument44 pagesList of service fees with dates and reference numbersMwenda MongweNo ratings yet
- Accounting For DepreciationDocument6 pagesAccounting For DepreciationKaran GNo ratings yet
- Simply Jordan TD Bank Statement Castillo Mar 2021Document2 pagesSimply Jordan TD Bank Statement Castillo Mar 2021MD MasumNo ratings yet
- ST8 Kcy464yDocument1 pageST8 Kcy464yIsmail NamutoroNo ratings yet
- ATLS Programme Draft 3Document2 pagesATLS Programme Draft 3Fernando GeldresNo ratings yet
- Assignment: Telecom Transmission & Switching TechniqueDocument14 pagesAssignment: Telecom Transmission & Switching TechniqueHAJRA khalidNo ratings yet
- Introduction To E-CommerceDocument3 pagesIntroduction To E-CommerceMartin MulwaNo ratings yet
- Eli Lilly's Project Resilience Case Study: Payers to Dictate Future of Pharma IndustryDocument17 pagesEli Lilly's Project Resilience Case Study: Payers to Dictate Future of Pharma IndustryYountekNo ratings yet
- Philippine School of Business Administration: Auditing (Theoretical Concepts)Document5 pagesPhilippine School of Business Administration: Auditing (Theoretical Concepts)John Ellard M. SaturnoNo ratings yet
- CISSP CASE ConceptDocument9 pagesCISSP CASE Conceptbabu100% (1)
- Proposal Business Plan Sistem Informasi Paket Wisata Nusa Penida Berbasis WebDocument25 pagesProposal Business Plan Sistem Informasi Paket Wisata Nusa Penida Berbasis Webayu riantiniNo ratings yet
- Research Paper - Roles of Commercial Bank in IndiaDocument9 pagesResearch Paper - Roles of Commercial Bank in Indiasalman.wajidNo ratings yet
- Bank Comfort Letter SampleDocument1 pageBank Comfort Letter SampleSunar Anom Arya Ganda100% (1)
- Chapter 11 Supplemental Questions: E11-3 (Depreciation Computations-SYD, DDB-Partial Periods)Document9 pagesChapter 11 Supplemental Questions: E11-3 (Depreciation Computations-SYD, DDB-Partial Periods)Dyan Novia67% (3)
- Kotak MahindraDocument43 pagesKotak MahindraUZARA KHANNo ratings yet
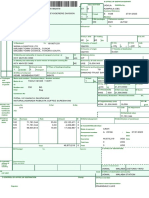
- Conhecimento de Embarque.Document2 pagesConhecimento de Embarque.Aleandro Vasconcelos NascimentoNo ratings yet
- CHAPTER 6 - The General Structure of Insurance IndustryDocument18 pagesCHAPTER 6 - The General Structure of Insurance Industryanis abdNo ratings yet