THE STATE OF RURAL HEALTH IN ILLINOIS:
Great challenges and a path forward
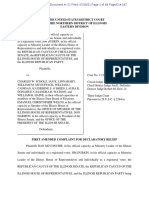
Small and Rural Hospital Locations Illinois has 102 counties and covers 57,914 square miles.
Our state is beautiful, dynamic, and populated by
innovative, caring, talented citizens. However, Illinois has
its challenges: disparities exist in the livelihood and
opportunities available for people living in the state’s
62 non-metropolitan counties. These differences result
in a much sicker rural and underserved Illinois compared
to its urban counterpart. Rural counties have higher rates
of smoking, obesity, child poverty and teen pregnancies
compared to urban counties. More uninsured adults live
in rural areas, causing rural hospitals to close and/or cut
vital services such as obstetrics care. Rural hospitals also
provide fewer mental health services. Therefore, Illinois’
rural residents are more likely to die from the five leading
causes of death than residents living in the state’s
metropolitan regions.
1.5 million Illinois residents live in the 62 non-metropolitan
counties. It is critically important to address rural Illinois
residents’ struggles to maintain healthy, active and
productive lives.
Authored by Illinois Rural Health
Summit Planning Committee
RuralHealthSummit@siumed.edu
THE RURAL HEALTH SUMMIT
On August 6-7, 2018, 50 influential stakeholders across various
sectors such as government, health care, public health, philanthropy
and academia met to share perspectives on the state of rural health in
Illinois. Organized by Southern Illinois University (SIU) School of
Medicine Department of Population Science and Policy, University of
Illinois at Chicago School of Public Health, SIU Paul Simon Public
Policy Institute, SIU School of Medicine Center for Rural Health and
Social Service Development and the Illinois Department of Public
Health, the goal of this two-day Rural Health Summit was to begin
building a blueprint to improve the social determinants of health in
rural Illinois through sustainable, innovative programs and policies.
KEY FINDINGS
Illinois’ rural communities have significant shortages in primary care physicians and
subspecialists, especially in mental health.
The shortage of a health workforce limits the ability of rural hospitals to find providers to care for
populations. 30.3 percent of small and rural hospitals are in designated primary care physician shortage areas.
93.7 percent of small and rural hospitals are in designated mental health service shortage areas.1
October 2018 The State of Rural Health in Illinois, page 2
Rate of patients receiving prescriptions for
Many of the highest rates of overdose deaths and opioid opioids andbenzodiazepine January 2017
prescriptions are in the rural counties of Illinois.
In 2016, Illinois had 1,946 deaths due to opioid overdoses,2 an 82
percent increase since 2013. The opioid-related death rate is 1.5 times
the rate of homicides and double the rate of deaths caused by
automobile accidents per year.
The neonatal abstinence syndrome (NAS) rate in rural counties
increased 212 percent from 2011 to 2015.3
In 2015, 8 million opioid prescriptions were filled in Illinois (60 opioid
prescriptions per 100 persons).4 Furthermore, injection drug use as
an HIV transmission risk factor accounted for a higher proportion of
diagnoses among persons living in rural counties compared to
non-rural counties (11 percent vs. 5 percent).5
Children in rural areas experience disadvantage
compared to urban children. A higher percentage
of children in rural areas experience financial
difficulties meeting basic needs.
A 2017 study found that almost 60 percent of
rural residents reported at least one Adverse
Childhood Experience (ACE) and 15 percent
experienced four or more ACEs. ACEs can lead to
higher risk of mental health disorder, prescription
drug use, suicide and negative physical health
outcomes.6,7 Only 48 percent of children in Illinois’
smaller, mostly rural counties attend
pre-kindergarten as compared to 55 percent of
their urban counterparts.8 A 2018 study by the
Illinois State Board of Education found that 75
percent of Illinois children are not prepared for
kindergarten.9
Source: Center for Disease and Control
Illinois’ geriatric population is growing exponentially. Readmission rates, social isolation
and limited health care services negatively affect the aging population.
The Illinois Department of Commerce and Economic Opportunity (DCEO) reported that the fastest growing
older population group is age 85 and older. DCEO projected the 85+ age group will total 402,311 people, an
increase of 109 percent, by 2030.10
Hospital location has a significant effect on readmissions. Patients discharged from rural hospitals are at 32
percent higher risk of unplanned readmissions as compared to those discharged from urban hospitals.11 The
study also found that patients discharged in rural areas had a 42 percent higher risk of unplanned
readmissions.
October 2018 The State of Rural Health in Illinois, page 3
Rural Illinois lacks nutrition and fitness education and practice, especially for youth,
resulting in increased rates of childhood obesity.
Poor nutrition and fitness are evident in rural areas where almost 33 percent of residents are classified as
obese. Rural Illinois residents lack safe outdoor spaces for physical activity.12
Food insecurity can permanently impair a child’s brain development, lower academic achievement and result
in more frequent hospitalizations. Conversely, children who regularly eat school breakfast score 18 percent
higher on standardized math tests,13 attend more days of school and are more likely to graduate from high
school. In Illinois, more than 800,000 students receive free or reduced price school lunch, but less than half
of those kids receive school breakfast,14 putting Illinois 42nd in providing school breakfast.15 Rural counties
consist of 63 percent of all counties in America but account for 85 percent of high child food-insecurity rate
counties.16
Housing quality plays a large part in physical and emotional well-being. Rural Illinois
struggles with housing quality and affordability.
Housing affordability empowers residents to own their own
home, relieving them of the stress associated with the
uncertainty of unstable housing. Poverty in rural areas
reached 14.5 percent in 2016 compared with 12.8 percent
in urban areas.18 Nearly 75 percent of housing stock in ru-
ral areas was built prior to 1980.19 Affordability is an issue in
rural areas; 25.1 percent of families spend between 30 and 49
percent of their income on monthly housing costs and 10.4
percent spend 50 percent or more.20 Nearly one in four rural
homes have been deemed “inadequate,” which poses multiple substantial threats to the tenant’s health,
including but not limited to lower utilization of medical care, higher use of the emergency room for
treatment, respiratory infections, psychological distress and cardiovascular disease.21, 22
Rural Illinois’ economy and healthcare system depend on each other. Strong
economies produce healthier residents; strong healthcare systems power economies.
Small and/or rural hospitals pump $2.5 billion into state and local economies via employee salaries and
benefits.23 Hospital employees generate $3.5 billion in economic activity in buying power in Illinois. These
hospitals create over 32,000 direct jobs and 42,000 indirect jobs in Illinois.24
October 2018 The State of Rural Health in Illinois, page 4
A PATH FORWARD: THE BEGINNINGS OF A BLUEPRINT
The health challenges faced in rural Illinois are daunting. However, public, corporate and community leaders
across rural Illinois are collaborating to help improve residents’ health. The following represents a sample of
the innovative ideas proposed by Rural Health Summit participants:
»» Expand high-speed broadband into rural areas to instantly create opportunities for higher quality access
to service. Currently, 37 percent of rural Illinois lacks broadband. High speed broadband internet can access
innovative learning techniques, online testing, remote learning and professional development for teachers
and administrators.25
»» Provide income tax credits to permanently endowed social funds to help support unmet rural health and
economic needs.
»» Invest in telepsychiatry and Medication Assisted Treatment (MAT) programs. MAT’s combination of FDA
approved medications with behavioral counseling has proven to reduce illicit opioid use and improve
patient adherence to treatment.26
»» Create public-private partnerships (government and rural health care systems) to recruit and retain a
health care and behavioral health workforce, including physicians, nurse practitioners, physician
assistants, social workers and behavioral therapists.
»» Create and improve programs to reduce the infant mortality rate: reinforce safe sleeping and home
visiting programs and increase the number of family physicians in rural areas.
»» Utilize rural hospitals as community hubs and create programs that link resident wellness and events
focused on community.
»» Revitalize the use of USDA programs such as the Single Family Housing Direct Home Loan program, the
514/516 Farm Labor Housing Loans and Grants, the Section 521 Rural Rental Assistance program and the
Section 538 Guaranteed Rural Rental Housing program.
»» Enhance communication and leverage existing partnerships between communities, caregivers and aging
patients, including utilizing telemedicine, integrated health homes and preventative and respite care.
October 2018 The State of Rural Health in Illinois, page 5
A CALL TO ACTION:
REINVESTMENT IN THE HEALTH OF RURAL ILLINOIS
We invite policymakers, corporate and community leaders across the state to join us in this important
work. Success will require partnerships, measures to effectively show progress and innovation that brings
lasting health outcome improvement.
Illinois faces important decisions in the months and years ahead. It is vital to consider the needs of rural
Illinois. Together, we can create the necessary momentum to more fully understand the health needs of our
residents, innovate with communities to create effective programs and sustain that health improvement with
policy change.
1 Illinois Health and Hospital Association (2018). Advancing Rural Health in Communities Across Illinois (1-19).
2 State of Illinois (2017). Comprehensive Opioid Data Report (1-38). Springfield, IL: State of Illinois.
3 Illinois Department of Public Health. Illinois Hospital Discharge Data. 2017.
4 https://www.drugabuse.gov/drugs-abuse/opioids/opioid-summaries-by-state/illinois-opioid-summary
5 IDPH. (2014). Illinois Enhanced HIV/AIDS Reporting System.
6 Radcliff, E., Crouch, E., & Strompolis, M. (2018). Rural–urban differences in exposure to adverse childhood experiences among South Carolina adults. Rural and Remote Health, 18(1).
7 https://www.samhsa.gov/capt/practicing-effective-prevention/prevention-behavioral-health/adverse-childhood-experiences
8 Christensen Gee, L., & Joseph, L. (2014). Disparities in Access to Preschool (1-31). Chicago, IL: Voices for Illinois Children.
9 Illinois State Board of Education (2018). KIDS Fall 2017 Data for Planning and Instruction (1-12). ISBE.
10 State of Illinois. State Plan on Aging: FY 2017 - FY 2019 (1-106). Illinois Department on Aging.
11 Toth, M., Holmes, M., Van Houtven, C., Toles, M., Weinberger, M., & Silberman, P. (2015). Rural Medicare Beneficiaries have Fewer Follow-up Visits and Greater Emergency Department Use
Postdischarge. Medical Care, 53(10), 908.
12 Toliver, Z. (2016). Building Rural Environments for Active Living. Retrieved from https://www.ruralhealthinfo.org/rural-monitor/built-environment-active-living/
13 Rise and Shine Illinois (2017). Powered by Breakfast: Healthy Starts in Illinois Schools (1-24). Chicago, IL: Greater Chicago Food Depository.
14 Rise and Shine. 1-24.
15 Philbin, E. M., & Rosso, R. (2018). School Breakfast Scorecard (1-21). Washington, D.C.: Food Research & Action Center.
16 Feeding America (2018). Map the Meal Gap 2018 - A Report on County and Congressional District Food Insecurity and County Food Cost in the United States in 2016 (1-75). Feeding America.
17 Scally, C., & Gilbert, B. (2018, October 02). Rural communities need more affordable rental housing. Retrieved from https://www.urban.org/urban-wire/rural-communities-need-more-af-
fordable-rental-housing
18 “Rural Health Information Hub.” Rural Health for Illinois - Introduction, 29 Nov. 2016, https://www.ruralhealthinfo.org/states/illinois.
19 Housing Assistance Council. (2012). Retrieved from http://www.ruraldataportal.org/index.aspx
20 Housing Assistance Council.
21 Housing Assistance Council.
22 Braveman, D., Egerter, S., & Pollak, C. (2018). Housing and Health. Retrieved May 1, 2011, from https://www.rwjf.org/en/library/research/2011/05/housing-and-health.html
23 Illinois Health and Hospital Association. 1-19.
24 Illinois Health and Hospital Association. 1-19.
25 Bjerga, A., & Hoffman, C. (2018, June 20). Democrats Take a Data-Driven Approach to Win Rural America. Retrieved from https://www.bloomberg.com/graphics/2018-rural-investment/
26 “Medication-Assisted Treatment Improves Outcomes for Patients With Opioid Use Disorder.” The Pew Charitable Trusts, Nov. 2016, https://www.pewtrusts.org/en/research-and-analysis/
fact-sheets/2016/11/medication-assisted-treatment-improves-outcomes-for-patients-with-opioid-use-disorder.
October 2018 The State of Rural Health in Illinois, page 6
You might also like
- Ruling by U.S. District Court On Illinois Legislative District Map Drawn by DemocratsDocument43 pagesRuling by U.S. District Court On Illinois Legislative District Map Drawn by DemocratsDean OlsenNo ratings yet
- Health Care Service Corp. Financial Statement 2020Document2 pagesHealth Care Service Corp. Financial Statement 2020Dean OlsenNo ratings yet
- Illinois Legislative Inspector General Resignation LetterDocument2 pagesIllinois Legislative Inspector General Resignation LetterDean OlsenNo ratings yet
- Lawsuit Challenging New Illinois Legislative District MapsDocument39 pagesLawsuit Challenging New Illinois Legislative District MapsDean Olsen100% (1)
- Latest Legal Complaint From Illinois GOP Legislative Leaders On RedistrictingDocument48 pagesLatest Legal Complaint From Illinois GOP Legislative Leaders On RedistrictingDean OlsenNo ratings yet
- Illinois House and Senate Democrats Release Revised Legislative MapDocument8 pagesIllinois House and Senate Democrats Release Revised Legislative MapDean OlsenNo ratings yet
- Springfield Clinic Letter To Patients On Dispute With Blue Cross and Blue Shield of IllinoisDocument2 pagesSpringfield Clinic Letter To Patients On Dispute With Blue Cross and Blue Shield of IllinoisDean OlsenNo ratings yet
- Request For Summary Judgment To Invalidate Illinois State Legislative District MapDocument21 pagesRequest For Summary Judgment To Invalidate Illinois State Legislative District MapDean OlsenNo ratings yet
- Letter From ACLU of Illinois To Springfield City Council On PanhandlingDocument3 pagesLetter From ACLU of Illinois To Springfield City Council On PanhandlingDean OlsenNo ratings yet
- Blue Cross and Blue Shield of Illinois Statement On Dispute With Springfield ClinicDocument2 pagesBlue Cross and Blue Shield of Illinois Statement On Dispute With Springfield ClinicDean OlsenNo ratings yet
- Heavily Redacted Documents From Earl Little's 2018 AutopsyDocument24 pagesHeavily Redacted Documents From Earl Little's 2018 AutopsyDean OlsenNo ratings yet
- Effective Dates of SAFE-T Act With Trailer Bill Changes June 2021Document5 pagesEffective Dates of SAFE-T Act With Trailer Bill Changes June 2021Dean OlsenNo ratings yet
- JB Pritzker, Governor Ngozi O. Ezike, MD, Director: MemorandumDocument2 pagesJB Pritzker, Governor Ngozi O. Ezike, MD, Director: MemorandumNewsTeam20No ratings yet
- Fall Covers For Spring Savings ProgramDocument2 pagesFall Covers For Spring Savings ProgramDean OlsenNo ratings yet
- Proposed Alterations To Illinois Cannabis LawDocument200 pagesProposed Alterations To Illinois Cannabis LawDean OlsenNo ratings yet
- Build Illinois Homes Tax Credit Fact SheetDocument2 pagesBuild Illinois Homes Tax Credit Fact SheetDean OlsenNo ratings yet
- COVID-19 and Disparities in Illinois Nursing HomesDocument14 pagesCOVID-19 and Disparities in Illinois Nursing HomesDean OlsenNo ratings yet
- Springfield Mayor Jim Langfelder State of The City Speech 2021Document23 pagesSpringfield Mayor Jim Langfelder State of The City Speech 2021Dean OlsenNo ratings yet
- Abraham Lincoln Presidential Museum Foundation's View of "Myth vs. Facts"Document3 pagesAbraham Lincoln Presidential Museum Foundation's View of "Myth vs. Facts"Dean OlsenNo ratings yet
- Testimony of Abraham Lincoln Presidential Library Foundation CEODocument5 pagesTestimony of Abraham Lincoln Presidential Library Foundation CEODean OlsenNo ratings yet
- State of Illinois Documents On Charles Hicks Jr.Document3 pagesState of Illinois Documents On Charles Hicks Jr.Dean OlsenNo ratings yet
- Testimony From Melissa Coultas, ALPLM Acting Executive DirectorDocument7 pagesTestimony From Melissa Coultas, ALPLM Acting Executive DirectorDean OlsenNo ratings yet
- Wrongful Death Complaint On Behalf of Family of Robert FolderDocument30 pagesWrongful Death Complaint On Behalf of Family of Robert FolderDean OlsenNo ratings yet
- Former Illinois State Historian Samuel Wheeler Report On Stovepipe Hat Possibly Owned by LincolnDocument54 pagesFormer Illinois State Historian Samuel Wheeler Report On Stovepipe Hat Possibly Owned by LincolnDean OlsenNo ratings yet
- Report On Illinois School For The DeafDocument60 pagesReport On Illinois School For The DeafDean OlsenNo ratings yet
- Illinois Historic Preservation Official Weighs in On Springfield YMCA PlansDocument2 pagesIllinois Historic Preservation Official Weighs in On Springfield YMCA PlansDean OlsenNo ratings yet
- Poll of Registered Voters On Abortion Notification Law For Minors in IllinoisDocument7 pagesPoll of Registered Voters On Abortion Notification Law For Minors in IllinoisDean OlsenNo ratings yet
- State ofDocument5 pagesState ofDean OlsenNo ratings yet
- Patients of Memorial Medical Center & ExpressCare Receiving Refunds On Debit CardsDocument2 pagesPatients of Memorial Medical Center & ExpressCare Receiving Refunds On Debit CardsDean OlsenNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- NSP2 PDFDocument92 pagesNSP2 PDFIrene C. CruzNo ratings yet
- Screening For Breast CancerDocument20 pagesScreening For Breast CancerqalbiNo ratings yet
- Changes in Central Corneal Thickness in Healthy Pregnant Women-A Clinical StudyDocument3 pagesChanges in Central Corneal Thickness in Healthy Pregnant Women-A Clinical StudyIJAR JOURNALNo ratings yet
- College DetailsDocument48 pagesCollege Detailsvivek chauhanNo ratings yet
- A J B P R: Sian Ournal of Iochemical and Harmaceutical EsearchDocument5 pagesA J B P R: Sian Ournal of Iochemical and Harmaceutical EsearchNAVNEET BAGGANo ratings yet
- Written Exam-2!2!2013Document1 pageWritten Exam-2!2!2013Charm MeelNo ratings yet
- G10 Health 1ST QuarterDocument32 pagesG10 Health 1ST QuarterDael GollaNo ratings yet
- Insights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityDocument4 pagesInsights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityHusnat hussainNo ratings yet
- Two Mechanisms of Hypertensive NephrosclerosisDocument2 pagesTwo Mechanisms of Hypertensive NephrosclerosisJessica Damasen Caballero0% (1)
- Juvenile Idiopathic Arthritis (Jia) : IAP UG Teaching Slides 2015-16Document15 pagesJuvenile Idiopathic Arthritis (Jia) : IAP UG Teaching Slides 2015-16KathirNo ratings yet
- Last health purchase, service used and who shared informationDocument17 pagesLast health purchase, service used and who shared informationRiccalhynne MagpayoNo ratings yet
- Breast and Nipple Thrush - 280720Document6 pagesBreast and Nipple Thrush - 280720Robbie WilliamsNo ratings yet
- Barge Clinic Visit Report SummaryDocument42 pagesBarge Clinic Visit Report SummaryNicoMichaelNo ratings yet
- Adrenaline - EpinephrineDocument3 pagesAdrenaline - Epinephrinesweety DangiNo ratings yet
- تجميعات باثولوجيDocument3 pagesتجميعات باثولوجيTurky TurkyNo ratings yet
- The Truth About The Flu ShotDocument5 pagesThe Truth About The Flu ShotPoorMexicanNo ratings yet
- Unknown PDFDocument3 pagesUnknown PDFSandy CastellanoNo ratings yet
- Health Apps - A ToolkitDocument3 pagesHealth Apps - A ToolkitAlexandra WykeNo ratings yet
- Teaching Plan for HypertensionDocument2 pagesTeaching Plan for HypertensionAno BaIto100% (1)
- Nursing Care of a Patient with AppendicitisDocument3 pagesNursing Care of a Patient with AppendicitisKeisha BartolataNo ratings yet
- Effectiveness of Massage and Manual Therapy'Document5 pagesEffectiveness of Massage and Manual Therapy'Kinjal SharmaNo ratings yet
- Andocor BrochureDocument19 pagesAndocor BrochureAffan AhmadNo ratings yet
- Cap MRDocument4 pagesCap MRKit BarcelonaNo ratings yet
- Visitor Health Declaration FormDocument2 pagesVisitor Health Declaration FormKaryl Eunice Macabale IboniaNo ratings yet
- Guide To Genetic CounselingDocument24 pagesGuide To Genetic Counselingmady_elenutza0% (1)
- How To Protect Yourself and OthersDocument2 pagesHow To Protect Yourself and OtherslistmyclinicNo ratings yet
- The Risk of Skin Reactions Using Ecg Electrodes 0711Document3 pagesThe Risk of Skin Reactions Using Ecg Electrodes 0711Benjamin DoverNo ratings yet
- List of Books For PurchaseDocument23 pagesList of Books For Purchasepavans25No ratings yet
- AssociationBetweenBRAFV600EMutationand MortalityDocument9 pagesAssociationBetweenBRAFV600EMutationand MortalityMade RusmanaNo ratings yet
- Govind AmbiGen PosterDocument1 pageGovind AmbiGen PosterYolanda MNo ratings yet