You might also like
- Howto Companion August2009Document4 pagesHowto Companion August2009lybrakissNo ratings yet
- Case Study: Management of A Patient With Primary Mediastinal B-Cell Lymphoma (PMBL)Document9 pagesCase Study: Management of A Patient With Primary Mediastinal B-Cell Lymphoma (PMBL)Bruce LennyNo ratings yet
- Medscape-Case Presentation Pediatric Non Hodgkin LymphomaDocument42 pagesMedscape-Case Presentation Pediatric Non Hodgkin LymphomaAnonymous 4b6BT9afNo ratings yet
- An Etiological Reappraisal of Pancytopenia - LargestDocument9 pagesAn Etiological Reappraisal of Pancytopenia - LargestKaye Antonette AntioquiaNo ratings yet
- Acute Lymphoblastic Leukemia ThesisDocument5 pagesAcute Lymphoblastic Leukemia Thesisljctxlgld100% (2)
- How I DiagnoseDocument17 pagesHow I DiagnoseFa FeNo ratings yet
- Principles of Oncology and Outline of ManagementDocument78 pagesPrinciples of Oncology and Outline of ManagementPavan JonnadaNo ratings yet
- Thesis On Hodgkin LymphomaDocument5 pagesThesis On Hodgkin Lymphomafjm38xf3100% (2)
- Ann Oncol-2014-Dreyling-iii83-92 PDFDocument10 pagesAnn Oncol-2014-Dreyling-iii83-92 PDFHessler Hannsen Zambrano CondoriNo ratings yet
- 2 +Hardi+and+Soeroharjo +analysis+of+hematologicalDocument6 pages2 +Hardi+and+Soeroharjo +analysis+of+hematologicalInnayah KhnisaNo ratings yet
- Lymphoma ThesisDocument8 pagesLymphoma Thesiszpxoymief100% (1)
- Fluid Complications: Malignant Pleural EffusionDocument11 pagesFluid Complications: Malignant Pleural Effusiont4tranNo ratings yet
- 368 FTP PDFDocument9 pages368 FTP PDFlPiNGUSlNo ratings yet
- Hodgkin lymphoma treatment and risksDocument9 pagesHodgkin lymphoma treatment and risksnandaNo ratings yet
- Journal Appraisal - TriadDocument43 pagesJournal Appraisal - TriadAmeerah MantawilNo ratings yet
- Diagnosis and Treatment Update - CholangiocarcinomaDocument4 pagesDiagnosis and Treatment Update - CholangiocarcinomaalfianfirdausNo ratings yet
- Guidelines for diagnosing childhood leukemiasDocument35 pagesGuidelines for diagnosing childhood leukemiasNarendraswari Mendina KusumawardhaniNo ratings yet
- Brock Et Al Liquid Biopsy 2015Document11 pagesBrock Et Al Liquid Biopsy 2015Jean BiverNo ratings yet
- Review Article: Biomarkers For Hepatocellular CarcinomaDocument8 pagesReview Article: Biomarkers For Hepatocellular CarcinomaAya AlkaffNo ratings yet
- Kolagocarsinoma PDFDocument7 pagesKolagocarsinoma PDFBerlyan RuslanNo ratings yet
- BR J Haematol - 2016 - Chaganti - Guidelines For The Management of Diffuse Large B Cell LymphomaDocument14 pagesBR J Haematol - 2016 - Chaganti - Guidelines For The Management of Diffuse Large B Cell LymphomaAdil EissaNo ratings yet
- Hodgkin's Lymphoma: A Guide to Diagnosis and TreatmentDocument6 pagesHodgkin's Lymphoma: A Guide to Diagnosis and Treatmentvictortayor_26105009No ratings yet
- Mantle Cell Lymphoma ThesisDocument7 pagesMantle Cell Lymphoma Thesisgjdpj4jq100% (1)
- Cancer Cytopathology - 2021 - Julien - Imprint Cytology Invaluable Technique To Evaluate Fresh Specimens Received in TheDocument13 pagesCancer Cytopathology - 2021 - Julien - Imprint Cytology Invaluable Technique To Evaluate Fresh Specimens Received in Theandynuransyah01No ratings yet
- Meningitis Workup - Approach Considerations, Blood Studies, Cultures and Bacterial Antigen TestingDocument14 pagesMeningitis Workup - Approach Considerations, Blood Studies, Cultures and Bacterial Antigen TestingdilaNo ratings yet
- Evaluation and Management of Suspected Sepsis and Septic Shock in AdultsDocument48 pagesEvaluation and Management of Suspected Sepsis and Septic Shock in AdultsIsmael IbrahimNo ratings yet
- Acute and Chronic in Ammation of The Biliary SystemDocument4 pagesAcute and Chronic in Ammation of The Biliary Systemfawzan mohammadNo ratings yet
- 19#prognostic HCC 2021Document7 pages19#prognostic HCC 2021hitashiNo ratings yet
- LeukemiaDocument10 pagesLeukemiaShapira alNo ratings yet
- Hepatocellular Carcinoma - Diagnosis and TreatmentDocument46 pagesHepatocellular Carcinoma - Diagnosis and TreatmentSigh BalaNo ratings yet
- Extracellular Nucleic Acids and Cancer: Michael - Fleischhacker@uk-Halle - de Bernd - Schmidt@uk-Halle - deDocument55 pagesExtracellular Nucleic Acids and Cancer: Michael - Fleischhacker@uk-Halle - de Bernd - Schmidt@uk-Halle - deAirin LeonieNo ratings yet
- Hepatocellular Carcinoma 2009Document58 pagesHepatocellular Carcinoma 2009ctsakalakisNo ratings yet
- Non-Hodgkin Lymphoma of The Breast: MD MD MD PHD MDDocument6 pagesNon-Hodgkin Lymphoma of The Breast: MD MD MD PHD MDlPiNGUSlNo ratings yet
- Pretreatment Leukocytes Predict Outcomes in HPV+ Oropharyngeal CancerDocument11 pagesPretreatment Leukocytes Predict Outcomes in HPV+ Oropharyngeal CancerJoana KellenNo ratings yet
- BCSH Diagnosis and Management of PlasmacytomasDocument14 pagesBCSH Diagnosis and Management of PlasmacytomasEva YustianaNo ratings yet
- Distal Cholangiocarcinoma (DCC) : Paxton V. Dickson, MD, Stephen W. Behrman, MDDocument57 pagesDistal Cholangiocarcinoma (DCC) : Paxton V. Dickson, MD, Stephen W. Behrman, MDALberta YosheNo ratings yet
- Sarcoidosis and Lymphoma Case Series and Literature ReviewDocument6 pagesSarcoidosis and Lymphoma Case Series and Literature Reviewea7sfn0fNo ratings yet
- Chronic Myeloid Leukemia Dissertation ThesisDocument7 pagesChronic Myeloid Leukemia Dissertation Thesiswendyboydsaintpetersburg100% (2)
- Pages 4 7Document4 pagesPages 4 7andreas_251650No ratings yet
- Baudin 2015Document24 pagesBaudin 2015barbara liuva chia policarpoNo ratings yet
- Ijlh 1251Document6 pagesIjlh 1251Ramadhan OlongNo ratings yet
- Pediatric Acute Lymphoblastic LeukemiaDocument9 pagesPediatric Acute Lymphoblastic LeukemiaAlvin PratamaNo ratings yet
- Int J Dermatology - 2015 - Bonchak - Calciphylaxis A Case Series and The Role of Radiology in DiagnosisDocument5 pagesInt J Dermatology - 2015 - Bonchak - Calciphylaxis A Case Series and The Role of Radiology in DiagnosisRichard LiuNo ratings yet
- Clinical Features of 37 Cardiac Lymphoma CasesDocument13 pagesClinical Features of 37 Cardiac Lymphoma CasesEmirza Nur WicaksonoNo ratings yet
- Lymphoma and HIVDocument20 pagesLymphoma and HIVALEX NAPOLEON CASTA�EDA SABOGAL100% (1)
- LLC 2006Document11 pagesLLC 2006claudia8a_ulamedNo ratings yet
- Portal Vein Thrombosis, Risk Factors, Clinical Presentation, and TreatmentDocument6 pagesPortal Vein Thrombosis, Risk Factors, Clinical Presentation, and TreatmentAdiNo ratings yet
- Liver Abscess DissertationDocument4 pagesLiver Abscess DissertationPayForAPaperAtlanta100% (1)
- 236 297Document8 pages236 297Andrea KamóNo ratings yet
- Get PDFDocument6 pagesGet PDFDarko MaksimovicNo ratings yet
- Lymphocelespostradicalj.1442 2042.2011.02797.xDocument6 pagesLymphocelespostradicalj.1442 2042.2011.02797.xarthurmathieuNo ratings yet
- American J Hematol - 2023 - Cheah-2Document14 pagesAmerican J Hematol - 2023 - Cheah-2salman mehriNo ratings yet
- Weber 2015Document12 pagesWeber 2015Nikos SerifisNo ratings yet
- A Literature Review of Complementary and Alternative Medicine Use by Colorectal Cancer PatientsDocument4 pagesA Literature Review of Complementary and Alternative Medicine Use by Colorectal Cancer Patientsgw0a869xNo ratings yet
- Ca de Colon y Polipos PDFDocument24 pagesCa de Colon y Polipos PDFGabriela Zavaleta CamachoNo ratings yet
- Botan's PE 2022Document69 pagesBotan's PE 2022Mimo HemadNo ratings yet
- CCCCCCCCCCCCCCCCCCCCCCCCCC C C ÷Document6 pagesCCCCCCCCCCCCCCCCCCCCCCCCCC C C ÷shaikameermalikNo ratings yet
- Disorders of Lymphatic SystemDocument43 pagesDisorders of Lymphatic SystemNurfanida Natasya MNo ratings yet
- Hematochezia in The Young Patient: A Review of Health-Seeking Behavior, Physician Attitudes, and Controversies in ManagementDocument7 pagesHematochezia in The Young Patient: A Review of Health-Seeking Behavior, Physician Attitudes, and Controversies in ManagementFelix Valerian HalimNo ratings yet
- Fast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsFrom EverandFast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsNo ratings yet
- Water Colored Splashes PowerPoint TemplateDocument36 pagesWater Colored Splashes PowerPoint TemplateAna Carmela DomingoNo ratings yet
- Kertas Resep YudiDocument1 pageKertas Resep YuditopNo ratings yet
- Abstrack Delibrate PracticeDocument2 pagesAbstrack Delibrate PracticetopNo ratings yet
- Pediatric Non-Hodgkin Lymphoma - Background, Etiology, EpidemiologyDocument11 pagesPediatric Non-Hodgkin Lymphoma - Background, Etiology, EpidemiologytopNo ratings yet
- Pediatric Non-Hodgkin Lymphoma Differential DiagnosesDocument2 pagesPediatric Non-Hodgkin Lymphoma Differential DiagnosestopNo ratings yet
- The Open Ophthalmology JournalDocument5 pagesThe Open Ophthalmology JournalFenny Duma SariNo ratings yet
- Slit LampbiomicrosDocument18 pagesSlit LampbiomicrostopNo ratings yet
- Eye TraumaDocument19 pagesEye TraumatopNo ratings yet
- Eye ManualDocument56 pagesEye Manualbashir019No ratings yet
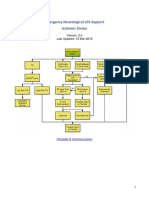
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Document22 pagesEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraNo ratings yet
- Pediatric Non-Hodgkin Lymphoma Medication GuideDocument8 pagesPediatric Non-Hodgkin Lymphoma Medication GuidetopNo ratings yet
- Pediatric Non-Hodgkin Lymphoma Treatment & Management: Approach ConsiderationsDocument15 pagesPediatric Non-Hodgkin Lymphoma Treatment & Management: Approach ConsiderationstopNo ratings yet
- Presentation 1Document8 pagesPresentation 1topNo ratings yet
- Radiologic Clinics of North America Volume 46 Issue 2 2008 (Doi 10.1016/j.rcl.2008.03.009) Abramson, Sara J. Price, Anita P. - Imaging of Pediatric LymphomasDocument26 pagesRadiologic Clinics of North America Volume 46 Issue 2 2008 (Doi 10.1016/j.rcl.2008.03.009) Abramson, Sara J. Price, Anita P. - Imaging of Pediatric LymphomastopNo ratings yet
- Pediatric Non-Hodgkin Lymphoma Clinical Presentation - History, Physical ExaminationDocument3 pagesPediatric Non-Hodgkin Lymphoma Clinical Presentation - History, Physical ExaminationtopNo ratings yet
- Antihistamines For Treating RhinosinusitisDocument6 pagesAntihistamines For Treating RhinosinusitistopNo ratings yet
- Role of PET/CT in Malignant Pediatric Lymphoma: Original ArticleDocument11 pagesRole of PET/CT in Malignant Pediatric Lymphoma: Original ArticletopNo ratings yet
- Role of Limited Whole-BodyDocument9 pagesRole of Limited Whole-BodytopNo ratings yet
- Nasal saline irrigation efficacy pediatric rhinosinusitisDocument19 pagesNasal saline irrigation efficacy pediatric rhinosinusitistopNo ratings yet
- CSS Jurnal DR IdratDocument8 pagesCSS Jurnal DR IdrattopNo ratings yet
- Total ModalDocument1 pageTotal ModaltopNo ratings yet
- Jurnal Asli CSS - Khalida Khairunnisa - DR - ErniDocument7 pagesJurnal Asli CSS - Khalida Khairunnisa - DR - ErnitopNo ratings yet
- Poster Publik & Poster IlmiahDocument10 pagesPoster Publik & Poster Ilmiahtop100% (1)
- Guideline AoeDocument25 pagesGuideline AoetopNo ratings yet
- DESIGN? VECTOR VS BITMAPDocument27 pagesDESIGN? VECTOR VS BITMAPtopNo ratings yet
- Antibiotics in Chronic RhinosinusitisDocument5 pagesAntibiotics in Chronic RhinosinusitistopNo ratings yet
- Felting Fabulous Flowers Templates PDFDocument3 pagesFelting Fabulous Flowers Templates PDFtop67% (3)
- Anatomy and Physiology Nasal ObstructionDocument13 pagesAnatomy and Physiology Nasal ObstructiontopNo ratings yet
- Role of Isotonic Saline Nasal Irrigation in Seasonal Allergic RhinitisDocument5 pagesRole of Isotonic Saline Nasal Irrigation in Seasonal Allergic RhinitistopNo ratings yet
- Chapter OneDocument36 pagesChapter Onebwire stephenNo ratings yet
- Development and Validation of HPLC Method For The Estimation of Lapatinib in Bulk Drugs and Pharmaceutical FormulationsDocument8 pagesDevelopment and Validation of HPLC Method For The Estimation of Lapatinib in Bulk Drugs and Pharmaceutical FormulationspalkybdNo ratings yet
- Life Saving Medicine PDFDocument15 pagesLife Saving Medicine PDFInTan PermataNo ratings yet
- The Signs and Symptoms of Testicular CancerDocument3 pagesThe Signs and Symptoms of Testicular Canceralvinperez12No ratings yet
- IT 1 - LIN Folic Acid & B12 Deficiency Anemia, Thalassemia & Hemoglobinopathia (BIOKIMIA)Document92 pagesIT 1 - LIN Folic Acid & B12 Deficiency Anemia, Thalassemia & Hemoglobinopathia (BIOKIMIA)Fakrocev Charlie GuloNo ratings yet
- PSM MCQDocument12 pagesPSM MCQGirish Waru50% (2)
- Contoh Esay Bahasa InggrisDocument3 pagesContoh Esay Bahasa InggrisWahyuniNo ratings yet
- Syllabus Oncology 2024Document6 pagesSyllabus Oncology 2024Kunal BhamareNo ratings yet
- Aplastic Anemia and HomoeopathyDocument3 pagesAplastic Anemia and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Xii English CoreDocument122 pagesXii English CoreShashwat Vyas0% (2)
- Kerala Medico Legal Code - Annexure2Document19 pagesKerala Medico Legal Code - Annexure2doctor82No ratings yet
- Locomotor System Study GuideDocument80 pagesLocomotor System Study Guidemartincorbacho100% (1)
- Union Christian College School of Health and Sciences City of San Fernando La UnionDocument11 pagesUnion Christian College School of Health and Sciences City of San Fernando La UnionJobelle AcenaNo ratings yet
- (Coll.) WHO Classification of Head and Neck Tumour (B-Ok - Xyz)Document285 pages(Coll.) WHO Classification of Head and Neck Tumour (B-Ok - Xyz)Andrea GonzalezNo ratings yet
- Revlon Case StudyDocument5 pagesRevlon Case StudyAriel Anthonie Puso GarciaNo ratings yet
- Balance The Imbalance: Diagnosis & Management of Vertigo - PresentDocument111 pagesBalance The Imbalance: Diagnosis & Management of Vertigo - PresentPraveen KumarNo ratings yet
- Dosis Ranitidin cw1Document5 pagesDosis Ranitidin cw1Cristine Indria Pieter IINo ratings yet
- 2008 04 Lecture 1 Interface Dermatitis FrishbergDocument6 pages2008 04 Lecture 1 Interface Dermatitis FrishbergYudistra R ShafarlyNo ratings yet
- Skin DisordersDocument4 pagesSkin DisordersAj PotXzs Ü100% (2)
- MSDS Light SpiritDocument9 pagesMSDS Light Spiritjhonni sigiroNo ratings yet
- The Basic Structure and Analysis of Medical TermsDocument100 pagesThe Basic Structure and Analysis of Medical TermsNadhira KartikaNo ratings yet
- Strategic Plan: Awareness Prevention TreatmentDocument16 pagesStrategic Plan: Awareness Prevention TreatmentAoy RangsimaNo ratings yet
- Cvs MnemonicsDocument3 pagesCvs MnemonicsSuneel Kaushik KNo ratings yet
- Circumcision Devices: A Review of Techniques and TechnologiesDocument43 pagesCircumcision Devices: A Review of Techniques and TechnologiesMakbruri Abdul AzizNo ratings yet
- DHEA PrasteronaDocument125 pagesDHEA PrasteronaMiguel Angel Contreras Ramos100% (1)
- Proximal Femur FracturesDocument34 pagesProximal Femur FracturesPrashant Madan MohanNo ratings yet
- Glossitis and Other Tounge Disorder PDFDocument12 pagesGlossitis and Other Tounge Disorder PDFMuhammad Iqbal Al-ayyubiNo ratings yet
- Knowledge of Cervical Cancer and Acceptance of HPVDocument6 pagesKnowledge of Cervical Cancer and Acceptance of HPVALIF FITRI BIN MOHD JASMINo ratings yet
- Alcoholic Drink - WikipediaDocument73 pagesAlcoholic Drink - WikipediaVaidehi chavankeNo ratings yet
- Not GlaucomaDocument5 pagesNot GlaucomaFabio LuccheseNo ratings yet