You might also like
- JournalDocument7 pagesJournalcarina adrianaNo ratings yet
- ACCF/AHA 2009 Expert Consensus Document On Pulmonary HypertensionDocument47 pagesACCF/AHA 2009 Expert Consensus Document On Pulmonary Hypertensioncarina adrianaNo ratings yet
- STANDARD PARASTERNAL AND APICAL TTE VIEWSDocument2 pagesSTANDARD PARASTERNAL AND APICAL TTE VIEWScarina adrianaNo ratings yet
- 2013 Cardiac Pacing and CRT 2013 ESC GuidelineDocument49 pages2013 Cardiac Pacing and CRT 2013 ESC GuidelineTony Gomez Luna LeyvaNo ratings yet
- Bradyarrhytmias CarinaDocument13 pagesBradyarrhytmias Carinacarina adrianaNo ratings yet
- JournalDocument7 pagesJournalcarina adrianaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Stress has pros and consDocument1 pageStress has pros and consMuhammad Aiman ZulhakimNo ratings yet
- FPGEE Blueprint: Area 1 - Basic Biomedical Sciences - 21%Document9 pagesFPGEE Blueprint: Area 1 - Basic Biomedical Sciences - 21%angelflairNo ratings yet
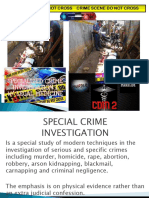
- Crime Scene Do Not Cross Crime Scene Do Not CrossDocument57 pagesCrime Scene Do Not Cross Crime Scene Do Not CrossMer BellezasNo ratings yet
- Simply Slim Weight Loss Guide: Hard Truths and The "Need To Know" Facts About Weight LossDocument7 pagesSimply Slim Weight Loss Guide: Hard Truths and The "Need To Know" Facts About Weight LossAaron SNo ratings yet
- Cirrus Health Presentation 0108dDocument10 pagesCirrus Health Presentation 0108dsureshnc23No ratings yet
- Don Mariano Marcos Memorial State University Campus Film Reveals Sugar's EffectsDocument3 pagesDon Mariano Marcos Memorial State University Campus Film Reveals Sugar's EffectsJinky FernandezNo ratings yet
- Root Cause Analysis Template 44Document3 pagesRoot Cause Analysis Template 44Devi ChintyaNo ratings yet
- DT-3000 SDS 090115Document8 pagesDT-3000 SDS 090115Alejandro VescovoNo ratings yet
- Northern Negros State College of Science and Technology: Republic of The PhilippinesDocument2 pagesNorthern Negros State College of Science and Technology: Republic of The PhilippinesKohi StrawberryNo ratings yet
- 6 DR NarsimuluDocument67 pages6 DR Narsimulushirish gundalaNo ratings yet
- Pancretic Cancer Case Study - BurkeDocument52 pagesPancretic Cancer Case Study - Burkeapi-282999254No ratings yet
- Faq City Ordinance 2020-059Document4 pagesFaq City Ordinance 2020-059WIS NewsNo ratings yet
- Meat Supply Chain Problems & SolutionsDocument8 pagesMeat Supply Chain Problems & SolutionstinuNo ratings yet
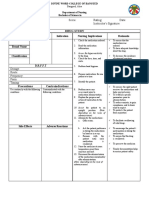
- Drug Study NCP Template 2Document2 pagesDrug Study NCP Template 2Janico Lanz BernalNo ratings yet
- NCP BreastfeedingDocument3 pagesNCP BreastfeedingLeo FrivaldoNo ratings yet
- 3060directory PDFDocument233 pages3060directory PDFtejasNo ratings yet
- 'Rrlyry: Ba) LRTDocument8 pages'Rrlyry: Ba) LRTMunish KumarNo ratings yet
- How To Stop SmokingDocument43 pagesHow To Stop SmokingRoselyn PacardoNo ratings yet
- Drug Study 2Document2 pagesDrug Study 2Joshua Selwyn SalazarNo ratings yet
- Human Energy Expenditure During Rest and Physical ActivityDocument46 pagesHuman Energy Expenditure During Rest and Physical ActivityKamyab Sadeghzadeh100% (2)
- Positive Body Image - (Chapter 1 - Body Image and Eating Issues)Document25 pagesPositive Body Image - (Chapter 1 - Body Image and Eating Issues)Micheal HasselNo ratings yet
- MRC Sujets Choisis 14 15Document50 pagesMRC Sujets Choisis 14 15Lamyaa IbnoozahirNo ratings yet
- Knowledge Attitudes and Practice of Community PharDocument16 pagesKnowledge Attitudes and Practice of Community Pharfirda amir parumpuNo ratings yet
- Acenocoumarol Drug Information, ProfessionalDocument47 pagesAcenocoumarol Drug Information, ProfessionalMoisés PonceNo ratings yet
- PHBIO lecture on DVT and PEDocument5 pagesPHBIO lecture on DVT and PEJamie Angelo PerezNo ratings yet
- Job Satisfaction of Nurses in Tarlac CityDocument4 pagesJob Satisfaction of Nurses in Tarlac CityAjeay PamintuanNo ratings yet
- Professional Meeting Reflective JournalDocument2 pagesProfessional Meeting Reflective Journalapi-430387359No ratings yet
- Case Study NCP ActualDocument3 pagesCase Study NCP Actualdhamy florNo ratings yet
- Music Therapy PsychiatryDocument59 pagesMusic Therapy PsychiatryAlberto ChicaybanNo ratings yet
- Babies With Birth DefectsDocument4 pagesBabies With Birth Defectsapi-307075288No ratings yet