You might also like
- Interpersonal Interaction and Personality Change in Group PsychotherapyDocument10 pagesInterpersonal Interaction and Personality Change in Group PsychotherapyDaniela UrreaNo ratings yet
- The Mindfulness Workbook For OCD A Guide To Overcoming Obsessions and Compulsions Using Mindfulness and Cognitive Behavioral Therapy PDFDocument234 pagesThe Mindfulness Workbook For OCD A Guide To Overcoming Obsessions and Compulsions Using Mindfulness and Cognitive Behavioral Therapy PDFThiago Brisolla96% (24)
- KkkduinnnsghsDocument1 pageKkkduinnnsghsDaniela UrreaNo ratings yet
- Trainees' Impressions of Psychotherapy and PsychotherapistsDocument8 pagesTrainees' Impressions of Psychotherapy and PsychotherapistsDaniela UrreaNo ratings yet
- Factors Related To Play Therapis Social Justice Advocacy Attitudes PDFDocument14 pagesFactors Related To Play Therapis Social Justice Advocacy Attitudes PDFDaniela UrreaNo ratings yet
- Implications of Psychotherapy Research For Psychotherapy TrainingDocument9 pagesImplications of Psychotherapy Research For Psychotherapy TrainingDaniela UrreaNo ratings yet
- Changes in Semantic Uses of First Person Pronouns As Possible Linguistic Markers of Recovery in PsychotherapyDocument7 pagesChanges in Semantic Uses of First Person Pronouns As Possible Linguistic Markers of Recovery in PsychotherapyDaniela UrreaNo ratings yet
- T He Dynamics of Change in PsychotherapyDocument7 pagesT He Dynamics of Change in PsychotherapyDaniela UrreaNo ratings yet
- Eriksonian Personality Research AndIts Implications For PsychotherapyDocument13 pagesEriksonian Personality Research AndIts Implications For PsychotherapyDaniela UrreaNo ratings yet
- Psychosocial Interventions For Self-Harm in AdultsDocument312 pagesPsychosocial Interventions For Self-Harm in AdultsDaniela UrreaNo ratings yet
- Self-Defining Memories, Scripts, Andthe Life Story Narrative Identity InPersonality and PsychotherapyDocument14 pagesSelf-Defining Memories, Scripts, Andthe Life Story Narrative Identity InPersonality and PsychotherapyDaniela UrreaNo ratings yet
- Negotiating A Pathological Identity in The Clinical Dialogue Discourse Analysis of A Family TherapyDocument19 pagesNegotiating A Pathological Identity in The Clinical Dialogue Discourse Analysis of A Family TherapyDaniela UrreaNo ratings yet
- Clients'and Therapists' Stories About Psychotherapy PDFDocument11 pagesClients'and Therapists' Stories About Psychotherapy PDFDaniela UrreaNo ratings yet
- Effectiveness of Psychotherapy in PersonalityDisorders Not Otherwise Speci Ed A Comparisonof Different Treatment ModalitiesDocument17 pagesEffectiveness of Psychotherapy in PersonalityDisorders Not Otherwise Speci Ed A Comparisonof Different Treatment ModalitiesDaniela UrreaNo ratings yet
- Exploring in Session Focus On ThePatient - Therapist Relationship PatientCharacteristics, Process and OutcomeDocument16 pagesExploring in Session Focus On ThePatient - Therapist Relationship PatientCharacteristics, Process and OutcomeDaniela UrreaNo ratings yet
- The Management of Polycystic Ovary Syndrome: Vincenza Bruni, Metella Dei, Valentina Pontello, and Paolo VangelistiDocument15 pagesThe Management of Polycystic Ovary Syndrome: Vincenza Bruni, Metella Dei, Valentina Pontello, and Paolo VangelistiDaniela UrreaNo ratings yet
- F (1 LJJ: LPLQL QDocument2 pagesF (1 LJJ: LPLQL QDaniela UrreaNo ratings yet
- Trainee Perspectives On Their Family Therapy TrainingDocument22 pagesTrainee Perspectives On Their Family Therapy TrainingDaniela UrreaNo ratings yet
- Pcos 1Document10 pagesPcos 1Daniela UrreaNo ratings yet
- Factors Related To Play Therapis Social Justice Advocacy AttitudesDocument14 pagesFactors Related To Play Therapis Social Justice Advocacy AttitudesDaniela UrreaNo ratings yet
- Therapeutics of The SelfDocument22 pagesTherapeutics of The SelfDaniela UrreaNo ratings yet
- (Asce) ST 1943-541X 0001117Document2 pages(Asce) ST 1943-541X 0001117Daniela UrreaNo ratings yet
- (Al-Luvial: Closure by Richard H. French 6Document4 pages(Al-Luvial: Closure by Richard H. French 6Daniela UrreaNo ratings yet
- The Politics of Gender in Family TherapyDocument17 pagesThe Politics of Gender in Family TherapyDaniela UrreaNo ratings yet
- Otra CosaDocument13 pagesOtra CosaDaniela UrreaNo ratings yet
- J. Hydraul. Eng., 1984, 110 (8) : 1179-1180Document2 pagesJ. Hydraul. Eng., 1984, 110 (8) : 1179-1180Daniela UrreaNo ratings yet
- Family Therapy and The Politics of EvidenceDocument23 pagesFamily Therapy and The Politics of EvidenceDaniela UrreaNo ratings yet
- Deconstructing Agnes - Externalization in Systemic SupervisionDocument11 pagesDeconstructing Agnes - Externalization in Systemic SupervisionDaniela UrreaNo ratings yet
- Feminism and Family Therapy-A Possible Meeting PointDocument16 pagesFeminism and Family Therapy-A Possible Meeting PointDaniela UrreaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 17 - Dr. Jarcia Vs People of The PhilippinesDocument16 pages17 - Dr. Jarcia Vs People of The PhilippinesColeen Navarro-RasmussenNo ratings yet
- Dextrocardia With Situs Inversus in An Adult Turkish 5797Document3 pagesDextrocardia With Situs Inversus in An Adult Turkish 5797Nazura Mohd NasirNo ratings yet
- PRSG Enlisted Candidate Application FormDocument11 pagesPRSG Enlisted Candidate Application FormJesus E. DelgadoNo ratings yet
- Transitions On The HorizonDocument38 pagesTransitions On The HorizonlandsomeNo ratings yet
- Upper Airway InfectionsDocument5 pagesUpper Airway InfectionsPhilline MacapagalNo ratings yet
- Bsbcmm401 Task 1 & 2 (Tal)Document16 pagesBsbcmm401 Task 1 & 2 (Tal)Shar KhanNo ratings yet
- SEEK Spotlight - Judith KonomahDocument3 pagesSEEK Spotlight - Judith KonomahMarisolNo ratings yet
- EPB 261 - Chemical Use and Storage at WaterworksDocument3 pagesEPB 261 - Chemical Use and Storage at WaterworksKONSTANTINOS TOMAZISNo ratings yet
- WMS 155+Installation+of+Cable+Tray+Document6 pagesWMS 155+Installation+of+Cable+Tray+monik_atabaresNo ratings yet
- Xi-Biden Summit: US Statement in FullDocument3 pagesXi-Biden Summit: US Statement in FullscmpNo ratings yet
- Titanium Dioxide SDS Safety Data SheetDocument7 pagesTitanium Dioxide SDS Safety Data SheetMauricioNo ratings yet
- Abdominal Injury2Document27 pagesAbdominal Injury2Worku KifleNo ratings yet
- 36 Pictures To See Which Muscle You'Re Stretching Make Your Life HealthierDocument14 pages36 Pictures To See Which Muscle You'Re Stretching Make Your Life HealthierGlenn Paul GalanoNo ratings yet
- Health Plan Financials ExplainedDocument467 pagesHealth Plan Financials Explainedvidya71v100% (1)
- Health Systems - DOH Affiliated AgenciesDocument66 pagesHealth Systems - DOH Affiliated AgenciesSeania BuenaventuraNo ratings yet
- Project Report On Herbal Extraction UnitDocument17 pagesProject Report On Herbal Extraction UnitEIRI Board of Consultants and PublishersNo ratings yet
- Pemanfaatan Drum Bekas Menjadi TangkiDocument17 pagesPemanfaatan Drum Bekas Menjadi TangkiChristina Mediana Cindy KhairaniNo ratings yet
- Basic Research in Orthopedic Surgery: Current Trends and Future DirectionDocument5 pagesBasic Research in Orthopedic Surgery: Current Trends and Future DirectionAyen Fajardo-HernalNo ratings yet
- Delhi WockhardtDocument92 pagesDelhi WockhardtnavdeepNo ratings yet
- Government Doctors in DelhiDocument408 pagesGovernment Doctors in DelhiBikki KumarNo ratings yet
- E-Ticket 1606210003846: Download Yatra AppDocument3 pagesE-Ticket 1606210003846: Download Yatra AppTathagataNo ratings yet
- ResearchDocument125 pagesResearchchittynagamaniNo ratings yet
- DDocument84 pagesDAwal BrosNo ratings yet
- The Centaur: Magazine From Centaur Services LimitedDocument28 pagesThe Centaur: Magazine From Centaur Services LimitedStela SilvaNo ratings yet
- ProvidersDocument110 pagesProvidersmaomao_vt89No ratings yet
- Sewa - 9 B PDFDocument3 pagesSewa - 9 B PDFTharunNo ratings yet
- Determination of Sulphite Sulphur Dioxide Thiosulphate and Thiocyanate With Notes On The Determination of Total Sulphur and Other Sulphur CompDocument69 pagesDetermination of Sulphite Sulphur Dioxide Thiosulphate and Thiocyanate With Notes On The Determination of Total Sulphur and Other Sulphur CompErika BenavidesNo ratings yet
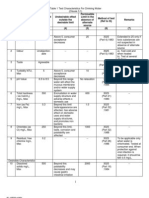
- Drinking Water - Is 10500-1991 PDFDocument3 pagesDrinking Water - Is 10500-1991 PDFearthanskyfriends100% (1)
- Brief Psychosocial Interventions For Substance AbuseDocument41 pagesBrief Psychosocial Interventions For Substance Abuseleeperlhan2000No ratings yet
- Fianna Fáil Ard Fheis Clar 2012Document108 pagesFianna Fáil Ard Fheis Clar 2012Politics.ieNo ratings yet