Professional Documents
Culture Documents
Ni Hms 383186
Uploaded by
Yaniatul AfdaCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Ni Hms 383186
Uploaded by
Yaniatul AfdaCopyright:
Available Formats
Fatigue in systemic lupus erythematosus:
Research
impact on occupational participation and
reported management strategies
Deirdre Connolly,1 Aine McNally,2 Deirdre Moran,3 and Margaret Ryan 4
Key words: Purpose: Fatigue is reported by approximately 81 per cent of people with systemic
Systemic lupus lupus erythematosus, with subsequent lower quality of life. Although standardized
erythematosus, measures have been used to examine the prevalence of fatigue, qualitative research
fatigue management, is needed to explore how people describe and cope with fatigue in their daily lives.
occupational participation. Method: Twelve people completed the Fatigue Impact Scale and were then
interviewed using semi-structured interviews. Data were analysed using descriptive
statistics and qualitative descriptive guidelines.
Findings: Participants were aged 22–62 years with a mean of 14.3 years
(SD 10) since diagnosis. Individual interviews identified an unpredictable pattern
of fatigue for the study participants and an impact on participation in occupations
of productivity and leisure, which resulted in loss of important life roles. Fatigue
management strategies were self-developed, with participants reporting no input
from health professionals.
Conclusion: The unpredictable nature of fatigue makes it difficult to manage.
It appears that development of both cognitive and practical strategies is required
to reduce the impact of fatigue on valued occupations. Early fatigue management
interventions could be beneficial for people with systemic lupus erythematosus in
order to manage this symptom. However, a larger study is required to confirm the
transferability of these findings.
1 Lecturer, Trinity College Dublin, Occupational
Therapy, St James’ Hospital, Dublin, Ireland.
2 Occupational Therapist, St
Dublin, Ireland.
James’ Hospital, Introduction
3 Occupational Therapist, Our Lady’s Hospice
Systemic lupus erythematosus (SLE) is a chronic, rheumatic, autoimmune
and Care Services, Occupational Therapy, disease. No single cause has been identified and the clinical presentation
Dublin, Ireland
4 Occupational Therapist, Enable Ireland,
ranges from a chronic debilitating disease to one that is potentially life threat-
Co. Meath, Ireland. ening due to organ dysfunction (D’Cruz 2006). Common symptoms include:
painful joints, fever, skin rash, chest pain, and chronic fatigue (Baker et al 2009,
Corresponding author: Deirdre Connolly, Scofield et al 2008). No epidemiological data are available on SLE in the Republic
Lecturer, Discipline of Occupational Therapy, of Ireland (RoI); however, there is a reported incidence rate of 4.71/100,000 of
Trinity Centre for Health Sciences, St James’ SLE in the United Kingdom (UK), with a higher rate of 7.62/100,000 in Northern
Hospital, James’ Street, Dublin 8, Ireland.
Ireland (NI) (Somers et al 2007). SLE is more prevalent among women, with
Email: deirdre.connolly@tcd.ie
a common age of onset between late teens and early 40s. Acute flare-ups of
Reference: Connolly D, McNally A, Moran D, SLE are managed with medication and rehabilitation (Brown 2006).
Ryan M (2014) Fatigue in systemic lupus SLE has a relatively low incidence within the general population in com-
erythematosus: impact on occupational parison to other inflammatory rheumatic conditions (Somers et al 2007). A
participation and reported management
need for research into specific issues in relation to SLE is required to assist
strategies. British Journal of Occupational
Therapy, 77(7), 373–380.
in planning and delivering suitable interventions for this population (Almehed
et al 2010). Fatigue is identified as a symptom of many chronic conditions which
DOI: 10.4276/030802214X14044755581862 interferes with occupational participation (Stout and Finlayson 2011). Law
(2002) defined occupational participation as the nature and extent of involve-
© The College of Occupational Therapists Ltd.
ment in activity, and stressed its importance for people with chronic conditions.
Submitted: 13 February 2013.
This exploratory study was aimed at investigating SLE-related fatigue,
Accepted: 9 April 2014.
including management strategies and impact on occupational participation.
British Journal of Occupational Therapy July 2014 77(7) 373
Downloaded from bjo.sagepub.com at KAI NAN UNIV on March 3, 2015
Fatigue in systemic lupus erythematosus: impact on occupational participation and reported management strategies
Literature review delivery of suitable interventions, this was considered a relevant
research design for this study.
A systematic review of quality of life in people with SLE reported
lower quality of life in people with SLE compared to other Participant recruitment
chronic conditions (Almehed et al 2010). Pain, fatigue, and Purposive sampling was used to recruit participants with
reduced ability to engage in work, social, and family activi- experience of the phenomenon being studied (Punch 2005).
ties are identified as the factors most strongly associated with Capturing and portraying a truly insider perspective of the
reduced quality of life in SLE (McElhone et al 2006, Thumboo research topic enhances authenticity of study findings in QD
and Strand 2007). Of these factors, 81% of people with SLE (Neergard et al 2009). Study participants were recruited
identified fatigue as the most debilitating symptom of their through a voluntary organization for people with SLE.
disease, which compromised participation in everyday activities Participant information letters were emailed to all members,
(Sohng 2003). inviting those who experience fatigue to participate in the
The impact of fatigue for women with a variety of chronic study. The first 16 people who responded to the email were
conditions was explored by Kralik et al (2005). The women contacted to establish their diagnosis of SLE (based on self-
described physical and psychological manifestations of fatigue. report) and their ability to participate in an interview. Of these
The authors concluded that, in addition to using quantifi- 16 people, three had other medical issues in addition to their
able measures of fatigue, it is important to capture subjec- SLE and were, therefore, excluded from the study. One other
tive descriptions. Other researchers have also highlighted person was unable to attend for interview due to travel diffi-
problems with fatigue measurement scales, stressing the culties. The remaining 12 people were recruited into the study.
need for personal accounts of fatigue (Rasker 2009). This Signed consent was returned to the researchers by post, along
legitimizes and validates people’s experiences of fatigue and with participants’ completed Fatigue Impact Scale (FIS, Fisk
increases healthcare providers’ understanding of it. et al 1994). Confidentiality was assured in the participant
There appears to be a gap in the literature with regard to information letter and the consent form. Ethical approval for
studies providing in-depth exploration of fatigue in SLE. the study was given by the Trinity College Dublin, Faculty of
Although Kralik et al’s study (2005) included women with Health Sciences Research Ethics Committee (17/07/2008).
SLE, it did not specifically investigate issues related to SLE
fatigue. It is unknown whether fatigue presents in a similar Data collection methods and process
pattern to other chronic conditions and what factors affect Two data collection approaches were utilized in this study.
and /or increase fatigue in SLE. Such information is important Study participants were initially asked to complete the FIS.
when planning and delivering suitable fatigue management This was done prior to their individual interviews to provide
interventions for people with SLE (Neill et al 2006). background information on their fatigue and act as a prompt-
This study, therefore, was an exploratory study aimed ing tool for the interviews, as self-report questionnaires have
at investigating: (1) experiences of and management strategies been recommended as a method of focusing discussions
for fatigue in SLE, and (2) the impact, if any, of fatigue on between researchers and research participants (Kielhofner
occupational participation. 2008). The FIS is a self-report tool that measures the impact
of fatigue on social, cognitive, and physical activities on a
4-point Likert scale. The total score ranges from 0 to 160, with
higher scores indicating higher impact of fatigue. A score of
Methods 75 and above indicates a significant impact of fatigue (Arnett
Study design and Rabinowitz 2010). The FIS has proven reliability and
The purpose of this exploratory study was to identify the validity for people who have chronic conditions with fatigue
nature and patterns of fatigue in SLE in order to inform the as a prominent symptom (Frith and Newton 2010).
design of suitable fatigue management interventions. The After reviewing and scoring the completed FIS, semi-
Medical Research Council (2008) recommended the use of structured interviews were arranged with each participant.
qualitative methods, in addition to quantitative and experi- The interview guide asked participants to describe their fatigue
mental methods, in designing and evaluating complex and to identify whether it impacted on their occupational
interventions. Qualitative description (QD), as described by participation, and if so, how. In QD semi-structured interviews
Sandelowski (2000), is a qualitative research design used to are used to elicit specific data in relation to the research aims
describe people’s perceptions and experiences of a particular (Milne and Oberle 2005). Interview duration was 40 to 85 min-
phenomenon. It is considered an appropriate methodology utes (median: 44.5 minutes, interquartile range 12.5 minutes).
for needs assessments and informing planning and delivery
of clinical interventions (Neergard et al 2009). A limitation Data analysis
of QD, however, is that, as it is not theory driven, and data In QD, the aim of data analysis is to provide a rich, straight
analysis is descriptive rather than interpretive, it reduces the description of an experience or event (Neergard et al 2009).
ability to make transferrable conclusions (Milne and Oberle QD analytical strategies were applied to the data. All inter-
2005). However, as the impetus for this study was to explore views were audio-recorded and fully transcribed. Interview
experiences of fatigue with a view to informing planning and transcripts were then transferred into N6 (NUD*IST 6), a
374 British Journal of Occupational Therapy July 2014 77(7)
Downloaded from bjo.sagepub.com at KAI NAN UNIV on March 3, 2015
Deirdre Connolly, Aine McNally, Deirdre Moran, and Margaret Ryan
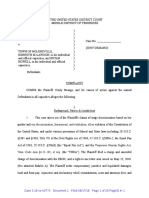
Table 1. Description of participants and total FIS scores
Study ID Gender Age (years) Age at diagnosis Time since diagnosis Work status FIS total score
P1 Female 62 54 8 Housewife 95
P2 Female 58 38 20 Volunteer 82
P3 Female 29 14 15 Full-time paid 120
P4 Female 37 25 12 Housewife 80
P5 Female 37 33 4 Self-employed 83
P6 Female 33 20 13 Full-time paid 48
P7 Male 58 32 26 Full-time paid 62
P8 Female 26 19 7 Part-time paid 37
P9 Female 38 35 3 Housewife 86
P10 Female 56 26 30 Housewife 117
P11 Female 22 18 4 Student 95
P12 Female 58 28 30 Resigned 92
Mean (SD) 42.8 (14.5) 14.3 (10) 83.1 (24.7)
software package from QSR International, used for analysis carried out by a team of researchers, rather than individuals,
of qualitative data. Interviews were conducted by under- facilitates authenticity and integrity (Punch 2005).
graduate final-year occupational therapy students, who had Neergard et al (2009) state that criticality is an important
varying experience of clients with fatigue through their practice element of authenticity. This was achieved through critical
education placements over a 4-year period. The first author analysis and continuous review of decisions made by members
of this research paper (MR), an occupational therapy lecturer of the research team. All decisions were documented, thereby
with considerable experience of working with clients with both providing an audit trail of the research process. This enables
inflammatory and non-inflammatory-related fatigue, super- replication of the study methodology, which contributes to
vised this study. authenticity (Miles and Huberman 1994).
All researchers coded a single interview independently In QD, integrity is important in reducing researcher bias
and then met to compare codes. Differences in codes were during data collection and data analysis (Sandelowski 2000).
discussed; where there was disagreement, codes were agreed Methods to achieve integrity included using evidence-based
on, re-named and /or new codes developed. The remaining literature to inform the research process, returning transcribed
eleven interviews were then allocated among the research interviews to study participants for member-checking, researcher
group and all agreed codes were applied to these interviews. triangulation during data analysis, and seeking participants’
Following this process, researchers met again, and any new validation of researchers’ summary of their data.
codes identified through individual analysis of the interviews
were discussed, agreed on, and, where appropriate, applied
across all interviews. On completion of the coding process
researchers grouped all codes into categories. These cate-
Findings
gories were then named to reflect the codes within each Twelve people (11 female) participated in this study. All
category. Categories were then grouped into their relevance participants were Caucasian, with ages ranging from 22 to
to the research objectives from which three themes related to 62 years and a mean of 14.3 years since diagnosis of SLE
fatigue in SLE were identified. In QD, identified themes clearly (SD 10 years). Table 1 provides demographic details on the
reflect the aims of the study (Neergard et al 2009). Transcripts participants and their total FIS score.
and summaries of individual interviews were returned to As can be seen from the FIS scores, the majority of partici-
participants to give them the opportunity to remove any infor- pants reported considerable fatigue with a mean FIS score
mation they were not willing to include, or to amend sum- of 83 (SD 24.7). The highest FIS scoring participant was P3,
maries of their transcripts if they did not feel it represented with a score of 120. Although this person works full-time,
their situation accurately. None of the participants made any which is likely a significant contributing factor in her total
changes to either their transcripts or summaries. FIS score, it is also interesting that she was the youngest person
Quantitative data from FIS were entered onto SPSS version in the group at time of diagnosis. This raises a potentially inter-
16 and analysed using descriptive statistics to provide an esting area for further research, which is whether there is a
overview of the extent of the impact of fatigue on study relationship between age of onset of SLE and levels of fatigue.
participants’ daily functioning. The total social, cognitive, and physical category scores
of the FIS are presented in Table 2. As there are 20 questions
Trustworthiness and rigour in the social category and ten questions in each of the other
Strategies for enhancing the rigour of QD have been outlined two categories, a ratio of 2:1 must be considered when com-
by Milne and Oberle (2005). In QD, researchers aim for paring category scores. Therefore, for this group, the greatest
authenticity and integrity of the research process. Studies impact of fatigue was on physical functioning.
British Journal of Occupational Therapy July 2014 77(7) 375
Downloaded from bjo.sagepub.com at KAI NAN UNIV on March 3, 2015
Fatigue in systemic lupus erythematosus: impact on occupational participation and reported management strategies
Table 2. Mean scores of FIS categories Occupational participation and associated roles
Category (score range) Mean score (SD) As it was an aim of the study to explore the impact of fatigue
Social (0–80) 41.99 (3.32) on occupational participation, this was an area much discussed
Cognitive (0–40) 17.41 (5.45) in all interviews. All participants identified a range of occu-
Physical (0–40) 23.55 (6.7) pations compromised due to their fatigue. As a result of restric-
Total FIS (0–160) 83.1 (24.7) tions on their occupations, the majority of participants also
discussed the impact of this on roles normally associated
with certain occupations.
Qualitative data analysis identified three themes: (1) the
nature of fatigue in SLE; (2) the impact of fatigue on occu- Occupational participation
pational participation and associated roles; and (3) fatigue Daily occupations are categorized as: self-care, work-related,
management strategies. or leisure (Law 2002). Of these three categories, self-care was
the least affected for all participants:
Nature of fatigue in SLE I’m fine with all that now but when I was first diagnosed I
This study purposefully recruited people who experienced found that a lot harder (P12).
fatigue as a result of SLE; therefore, all participants reported
experiencing fatigue to varying levels and identified it as their Well to be honest, it was never a problem (P4).
worst symptom: Work-related and leisure occupations presented difficulties
Fatigue is the one symptom that affects my life the most. It’s for all participants. All 12 participants were below the generally
the symptom that stops me doing things I want to do and it is recognized retirement age, in the UK, of sixty-five. Five partici-
the hardest to cope with (P11). pants worked outside the home in either full- or part-time
employment. Of the remaining seven, one was in full-time
You’re so tired that you have nothing left to give. It means you
education and the other six worked inside the home. All par-
have no energy left to give anything back. What I say is if you
ticipants discussed the impact of fatigue on paid and unpaid
put me in a coffin and closed the lid I’d have said thank you
work-related activities. For those in paid employment, flexi-
very much, I’m very happy, I’m that tired (P10).
bility and a supportive employer were critical factors in main-
Participants reported a wide variety to the pattern of their taining employment:
fatigue. Ten participants discussed its unpredictability:
I have an excellent boss who’s very approachable and under-
Fatigue can arrive out of the blue. It’s a tiredness that comes standing. My career is organized so I only ever have to work
over you and you have to go to bed. I could have it very bad 22 hours-a-week (P8).
for a week or two and then for the past month I haven’t been
as tired at all (P1).
Participants discussed ways in which they modified work
activities in order to remain in employment. Such modifi-
… it can be very bad for a day or two and then all of a sudden cations included working part time, looking for work closer
it goes away (P2). to home, and using time in work constructively in order to
For some participants fatigue is always present, even avoid taking work home in the evenings or weekends. One
after rest periods. P8 described waking in the morning as participant chose her current studies based on the potential
‘looking for the track marks as if something ran over me’. future demands of her work:
In other chronic diseases, such as multiple sclerosis,
… the environment that I will end up working in, for example
fatigue is reported as a constant symptom (Smith and Hale
in an office, will be better for me. At least I can sit down all day
2007). However, some of the participants reported long
(P11).
periods both with and without fatigue:
Household chores also caused difficulty for the majority
It can vary so much from day to day. I could go weeks and I
of participants, with tasks such as preparing meals, cleaning,
am fine. Then I have weeks where I am very tired. I have never
shopping, laundry, and gardening identified as problematic:
even noticed a pattern to it to be honest (P4).
For instance, cleaning the house, I had to get cleaners in (P5).
The three most common factors that increased participants’
fatigue were stress, physical activity, and joint pain, with Take for example the garden — I would have been in full
stress being the most commonly discussed. P12 explained that control before but now I need help from others emptying the
‘Stress really makes the fatigue worse’ and P1 that ‘Stress grass, trimming the hedges, that sort of thing. I used to be able
takes twice as much out of me’, while P11 described stress to do all that myself, but not anymore (P7).
and fatigue as ‘a vicious circle’. P10 explained ‘you cannot On discussing leisure activities, eleven of the participants
reduce the fatigue until you relieve the stress’. This analogy identified changes they had made, such as stopping certain
of a vicious circle was also applied to pain and fatigue, as activities, taking up less physically demanding leisure pur-
described by P8: suits, or altering them to accommodate fatigue. P9, who does
When I’m having joint pain, I’m more fatigued, and if I’m more not drive, said ‘by the time I walk to the gym I don’t have the
fatigued, I’m going to have joint pain (P8). energy levels to do anything’, while others commented:
376 British Journal of Occupational Therapy July 2014 77(7)
Downloaded from bjo.sagepub.com at KAI NAN UNIV on March 3, 2015
Deirdre Connolly, Aine McNally, Deirdre Moran, and Margaret Ryan
I was big into cycling, swimming, and camogie but I’ve had I’ve learned to live with it and become more positive. That is
to give them all up (P11). one of the major things I have to work with on a daily basis is
positive thinking (P4).
I played badminton but I gave that up for fatigue reasons and
joint pain (P8). I have become a more mellow person and so now I try to let
things wash over me because if I get worried or stressed it
Some participants described how they have developed
doesn’t do me any favours (P12).
new leisure interests that are not as fatiguing. P9 identified
walking as a leisure activity she now enjoys: You can’t get as involved as you might like to. The old me would
have been stuck in the middle of it all. The new me is more
We live right beside the beach and I find that very relaxing. reserved (P9).
It’s easy on the joints (P9).
Participants also spoke of changing their attitudes in
P11 explained how yoga and Pilates helps in reducing relation to what they considered important in their lives.
her fatigue: For example, due to limited energy levels, P12 made choices
… you benefit from the rest and the relaxation (P11). between spending time with family or friends:
It was a case of if I wanted to be okay during the day for the
Impact of occupational restrictions on roles children and my husband, then going out in the evenings
As a result of reduced ability to participate in valued occu- was not an option. I couldn’t have both so I chose what was
pations, participants discussed the impact this had on what more important to me (P12).
they considered important life roles. These role-adjustments
Another cognitive adjustment identified was how partici-
were as a result of changes made to paid work and leisure
pants altered their expectations of themselves:
activities, and included changes to the role of mother, daughter,
child-minder and volunteer. I used to think ‘I must have the house clean, I must have this
One participant identified the impact of fatigue on her done, I must have that done, I must be the perfect person’.
relationship with her son: But now I say ‘you can do that tomorrow’. But it took years
for me to realize that (P10).
When it was really bad I wasn’t able to do anything and my
husband kind of took over. So, when he was here he did every- Becoming more adaptable involved participants learning
thing with my son and as a result of that my son wanted to to do things differently and be more flexible
be with him all the time and that was really hard (P5). I’ve learned through experience to pace myself, take it easier,
Another explained how she could no longer look after and rest a little bit if I want to do something. If I want to go
her grandsons: to a function, I go to bed for an hour or two before (P7).
I would love to be able to look after the two lads. Grannies External supports
are supposed to look after their grandkids but I wouldn’t be External supports for managing and reducing fatigue involved
able to do that (P1). taking up activities generally recognized as stress-relieving
Being unable to participate in certain sport activities has and relaxing, and getting help and support from family and
changed how P11 and her father spend their time together: friends. None of the participants discussed input from health
professionals on managing their fatigue.
With my dad, he is really sporty and loves the outdoors. It was A range of complimentary therapies including yoga, Pilates,
always me and my dad that did things together. He used to come meditation, acupuncture, and massage were employed by
to all my camogie games, we would go cycling every Sunday seven participants. These participants identified how this
and we climbed together. I mean, we are still as close but it has helped them to relax, thereby reducing their fatigue. However,
changed what I do with him. one participant (P8) who had tried a number of complimen-
tary approaches reported that pacing her activities was the
Fatigue management strategies most effective for her.
Participants discussed a variety of strategies for managing Family, friends, neighbours, and members of support
their fatigue in order to enable them to participate in valued groups were identified as providing invaluable support and
occupations. These strategies were developed over time as practical help. This support ranged from hands-on help with
participants learned to accommodate their SLE and become housework and childcare to emotional support:
familiar with the patterns of their fatigue. Reported strategies
My partner is brilliant. He works full time. He comes home
are grouped into intrapersonal strategies and external supports.
and cooks the dinner every day. I’m so lucky he understands
my illness, and doesn’t get annoyed or irritated with me being
Intrapersonal strategies
tired all the time (P8).
Intrapersonal management strategies involved periods of
cognitive adjustments where participants discussed ‘accepting’ My sisters are great. They understand my mood swings and the
their limitations followed by a shift of focus from limitations whole lupus thing. I know some people think that I am lazy
to abilities: but my family understands what I am going through (P4).
British Journal of Occupational Therapy July 2014 77(7) 377
Downloaded from bjo.sagepub.com at KAI NAN UNIV on March 3, 2015
Fatigue in systemic lupus erythematosus: impact on occupational participation and reported management strategies
In summary, fatigue was described as an unpredictable who were working also identified the importance of support
and constant feature of SLE. Many factors were identified as from their employers; however, not all received the same
increasing fatigue, with stress being most frequently discussed. level of support. This indicates the importance of educating
Fatigue affected a wide range of occupations, with work and employers on the impact of fatigue on productivity levels and
leisure most frequently identified. Continued participation in on strategies that can be used in the workplace to manage
employment required modifications to work routines and work fatigue. These can include making changes to work environ-
environments. Participants discussed needing to be organized ments to reduce the energy output for employees with SLE or
but at the same time flexible in order to manage their fatigue. other fatigue-related diseases. The need for direct interventions
None of the participants reported having received interven- to reduce work-related disabilities has also been recognized
tions for fatigue management from health professionals. in Canadian research (Somers et al 2007). This could include
work-specific fatigue management programmes, which
identify strategies for managing fatigue in the workplace.
In the interviews, home-based occupations were also
Discussion identified as increasing fatigue, with many seeking assistance
An episodic and unpredictable pattern of fatigue was from family members. This was also evident in high scores
described by study participants, highlighting that this might on an item of the FIS social category ‘I have to rely on others
be a common feature of fatigue in SLE. However, this needs to help or do things for me’. Energy conservation strategies
further research to establish whether others with SLE report for people with fatigue-related chronic conditions, as out-
similar patterns to their fatigue. The episodic and inter- lined by Stout and Finlayson (2011), such as delegating or
mittent nature of fatigue reported by the study participants altering methods for completing activities, may, therefore,
appears to be different from the more predictable pattern of be helpful. Additionally, those with SLE may need guidance
other chronic conditions such as multiple sclerosis (MS) (Smith in prioritizing valued occupations and accepting help for
and Hale 2007). This, therefore, makes it more difficult for low priority activities. Making these decisions appears to be
the study participants to plan activities ahead of time or to an important element of the attitudinal changes, identified
apply pre-established strategies for managing their fatigue. in this study, which are required to manage fatigue.
If this finding is validated through a larger study, it could Self-care and work-related occupations are often priori-
be important information to include in fatigue management tized over leisure occupations by people with chronic con-
education so that others are prepared for potential episodes of ditions (Cahill et al 2010). However, the importance of
sudden onset fatigue and learn to not be self-critical if planned engaging in leisure activities for physical and mental well-
activities have to be altered or cancelled. Participants also being has been clearly documented (Paganini-Hill et al 2011).
discussed long periods without fatigue followed by a sudden In this study, the majority of participants continued to under-
onset of fatigue, indicating a need for ongoing education on take some form of leisure activities although they identified
effective fatigue management for the study participants. having changed their leisure interests from physical-based to
In the interviews, stress, joint pain, and physical activities more sedentary activities. This supports the value attached
were all factors identified as increasing fatigue. Participants to leisure participation and, consequently, the importance of
discussed the importance of managing stress in order to occupational therapists addressing this area early post-diagnosis
reduce fatigue. This was also a finding in the social category so that assistance can be given in maintaining involvement
of the FIS, with high scores from participants on the item in leisure activities.
‘I avoid situations that are stressful for me’. Strategies for
managing stress are often included in fatigue management Fatigue management strategies
programmes (Connolly et al 2013). Increasing awareness Fatigue management strategies varied among study partici-
of other factors that increase fatigue, such as joint pain and pants. All discussed internal and external strategies to manage
physical activity, may also need to be highlighted in fatigue fatigue. External strategies are similar to those used by people
management education for people with SLE. with other chronic diseases such as MS and arthritis-based
With respect to occupational participation, participants diseases (Harrison 2007, Kralik et al 2005). What came out
identified most difficulties with work and leisure occupations. frequently, however, was the range of cognitive strategies
In this study, five of the 12 participants were involved in and attitudinal adjustments that the study participants made
some degree of paid employment. It has been estimated that to accommodate their fatigue.
only half of people with SLE remain in employment, resulting The participants discussed how, over time, they changed
in the majority of the economic costs associated with SLE how they viewed their disease. They described accepting
(Almehed et al 2010). A greater tendency towards sedentary limitations imposed by the disease process and accepting
work was reported by Almehed et al (2010) for people with help from others. They also identified the importance of
SLE compared to the general population. In this study, two changing from complaining about their disease to taking a
participants changed from nursing to office-based careers, positive attitude and being flexible in relation to what they
which better suited their fatigue levels. This finding aligns achieve over the course of their day. This flexibility appears
with high scores on the item ‘ability to sustain physical to be important in managing the unpredictability of SLE-related
activity’ on the FIS physical functioning category. Participants fatigue, which participants identified when describing the
378 British Journal of Occupational Therapy July 2014 77(7)
Downloaded from bjo.sagepub.com at KAI NAN UNIV on March 3, 2015
Deirdre Connolly, Aine McNally, Deirdre Moran, and Margaret Ryan
nature of their fatigue. This change in attitude could be viewed arthritic diseases. Therefore, perhaps it lacks prioritization
as ‘giving in’ to occupational limitations caused by fatigue. among health professionals. Further research is required to
However, perhaps a more positive way of considering this explore this possibility.
is as an empowering approach to managing fatigue, of It is hoped that this study contributes to an increased
taking control of the disease rather than the disease taking understanding of fatigue in SLE. The findings suggest that,
control of the person. Strategies for making these attitudinal unlike other chronic diseases, fatigue in SLE does not present
changes could be included in fatigue management pro- with a consistent pattern. It is, perhaps, this unpredictability
grammes for people with SLE. Cognitive behavioural that makes it a particularly difficult symptom to manage.
strategies facilitate changes in a person’s thinking patterns However, further research is needed to confirm this finding.
to impact positively on their behaviours (Early 2000). Using This study has also highlighted the role of cognitive and atti-
such an approach in fatigue management education, occupa- tudinal strategies in managing fatigue, in addition to practical
tional therapists could facilitate attitudinal changes to fatigue approaches. These are, therefore, important components to
in order to increase participation in valued occupations. include in fatigue management education and interventions
Participants also discussed shifting priorities within for people with SLE.
their personal lives as another way of managing fatigue.
When energy levels are low or limited, choices have to be
made about how to use energy efficiently. Literature in Key findings
relation to energy management discusses setting priorities ■ For the participants of this study, fatigue in SLE was reported as
in relation to occupational participation, and making unpredictable and impacting mainly on productivity and leisure.
choices regarding when and how occupations are performed ■ A combination of intrapersonal and external strategies was used by
(Smith and Hale 2007). However, the participants in the study participants to manage their fatigue.
current study also discussed making priorities in relation
to with whom they choose to spend time. They spoke of What the study has added
choosing family members over friends or engaging in This study contributes towards an increased understanding of fatigue in
social activities. These attitudinal and emotional decisions SLE and has indicated a need for early fatigue management interventions
appear to be an important element of managing fatigue in for people with SLE.
SLE. It is interesting to note that none of the participants in
this study received any input from healthcare professionals
in recognizing the need to make these cognitive adjustments. Conflict of interest: None declared.
Perhaps such input would help in making what can be diffi- Funding: This research received no specific grant support from any funding
cult decisions earlier in the disease trajectory, thereby avoid- agency in the public, commercial, or not-for-profit sectors.
ing having to withdraw completely from work and valued Research ethics: Ethical approval for the study was given by the Health
leisure activities. Sciences Research Ethics Committee, Trinity College, Dublin (REF NUMBER
Many study participants discussed difficulty accessing TO COME).
fatigue-specific information when diagnosed with SLE. As
a result, the majority of their fatigue management strategies References
were acquired through trial and error and talking with others Almehed K, Carlsten H, Forsblad-d’Elia H (2010) Health-related quality of life
with SLE on an ad hoc basis. This is similar to the Australian in systemic lupus erythematosus and its association with disease and work
study whose participants also spoke of lack of education and disability. Scandinavian Journal of Rheumatology, 39(1), 58–62.
guidance immediately post-diagnosis (Kralik et al 2005). Arnett PA, Rabinowitz AR (2010) The neuropsychological presentation and
These findings support early and timely interventions from treatment of demyelinating disorders. In: JM Gurd, U Kischka, JC Marshall,
health professionals on the nature of fatigue in SLE and eds. The Handbook of Clinical Neuropsychology. Oxford: Oxford Press,
appropriate fatigue management strategies. 585–605.
Baker K, Pope J, Fortin P, Silverman E, Peschkin C, 1000 Faces of Lupus Investigators,
CaNIOS (2009) Work disability in systemic lupus erythematosus is prevalent
and associated with socio-demographic and disease related factors. Lupus,
Conclusion 18(4), 1281–1288.
This study provides personal accounts of how fatigue in SLE Brown SJ (2006) Practical approaches to managing lupus. Practice Nurse,
affects occupational participation. However, a limitation of 32(1), 26–29.
the study is that, as it was not a clinical-based sample, medical Cahill M, Connolly D, Stapleton T (2010) Exploring occupational adaptation
confirmation was not available with respect to participants’ through the lives of women with multiple sclerosis. British Journal of
fulfilment of SLE diagnostic criteria or pathology of their Occupational Therapy, 73(3), 106–115.
lupus. Therefore, their fatigue may be related to a different Connolly D, O’Toole L, Redmond S, Smith S (2013) Managing fatigue in
health issue. Despite this, however, the findings indicate that patients with chronic conditions in primary care. Family Practice, 30(2),
fatigue is problematic for these participants and impacts 123–124.
on many facets of their lives. SLE is not a widely prevalent D’Cruz DP (2006) Systemic lupus erythematosus. British Medical Journal,
disease, particularly when compared to other inflammatory 332(7546), 890–894.
British Journal of Occupational Therapy July 2014 77(7) 379
Downloaded from bjo.sagepub.com at KAI NAN UNIV on March 3, 2015
Fatigue in systemic lupus erythematosus: impact on occupational participation and reported management strategies
Early MB (2000) Medical and psychological models of mental health and illness. Neill J, Belan I, Ried, K (2006) Effectiveness of non-pharmacological interventions
In: Mental health concepts and techniques for the occupational therapy for fatigue in adults with multiple sclerosis, rheumatoid arthritis, or systemic
assistant. 4th ed. Philadelphia: Lippincott Williams & Wilkins. 17–43. lupus erythematosus; a systemic review. Journal of Advanced Nursing,
Fisk JD, Ritvo PG, Ross L, Haase DA, Marrie J, Schelch WF (1994) Measuring 56(6), 617–635.
of functional impact of fatigue: Initial validation of the Fatigue Impact Paganini-Hill A, Kawas C, Corrada MM (2011) Activities and mortality in
Scale. Clinical Infectious Diseases, 18(Supplement 1), S79–S83. the elderly: the Leisure World cohort study. The Journals of Gerontology,
Frith J, Newton J (2010) Fatigue Impact Scale. Occupational Medicine, 60(2), 159. 66(5), 559–567.
Harrison S (2007) Fatigue management for people with multiple sclerosis. Punch K (2005) Introduction to social research: quantitative and qualitative
London: College of Occupational Therapists. approaches. SAGE: London.
Kielhofner G (2008) Self-reports: eliciting client’s perspectives. In: Model of Rasker JJ (2009) The enigma of fatigue. The Journal of Rheumatology, 36(12),
human occupation: theory and application. 4th ed. Lippincott Williams 2630–2632.
& Wilkins. 237–261. Sandelowski M (2000) Whatever happened to qualitative description? Research
Kralik D, Telford K, Price K, Koch T (2005) Women’s experience of fatigue in in Nursing and Health, 23(4), 334–340.
chronic illnesses. Journal of Advanced Nursing, 52(4), 372–380. Scofield L, Reinlib L, Alarcon GS, Cooper GS (2008) Employment and disability
Law M (2002) Participation in the occupations of everyday life. American issues in systemic lupus erythematosus: a review. Arthritis & Rheumatism,
Journal of Occupational Therapy, 56(6), 640–649. 59(10), 1475–1479.
McElhone K, Abbott J, Teh LS (2006) A review of health related quality of Smith C, Hale L (2007) The unique nature of fatigue in multiple sclerosis:
life in systemic lupus erythematosus. Lupus, 15(10), 633–643. prevalence, pathophysiology, contributing factors and subjective experience.
Medical Research Council (2008) Developing and evaluating complex Physical Therapy Review, 12(1), 43–51.
interventions: new guidance. Available at: http://www.mrc.ac.uk/documents/ Sohng KY (2003) Effects of a self-management course for patients with systemic
pdf/complex-interventions-guidance/ Accessed 26.06.14. lupus erythematosus. Journal of Advanced Nursing, 42(5), 479–486.
Miles MB, Huberman AM (1994) Qualitative data analysis: An expanded Somers EC, Thomas LS, Schoonen WM, Hall AJ (2007) Incidence of systemic
sourcebook. Thousand Oaks: SAGE Publications. lupus erythematosus in the United Kingdom, 1990-1999. Arthritis &
Milne J, Oberle K (2005) Enhancing rigor in qualitative description: a case study. Rheumatism, 57(4), 612–618.
Journal of Wound, Ostomy and Continence Nursing, 32(6), 413–420. Stout K, Finlayson M (2011) Fatigue management in chronic illness. American
Neergard MA, Olesen F, Andersen RS, Sondergaard (2009) Qualitative description Occupational Therapy, 24(1), 16–19.
– the poor cousin of health research? BMC Medical Research Methodology, Thumboo J, Strand V (2007) Health-related quality of life in patients with
9(52), 1–5. Available at: http://www.biomedcentral.com/1471-2288/9/52 systemic lupus erythematosus: an update. Annals Academy of Medicine
Accessed 13.09.12. Singapore, 36(2), 115–122.
Jackie Pool
Call for papers Dr Lesley Collier
Special Issue — Dimensions of dementia: the unique contribution of occupational therapy
The Editorial Board of the British Journal of Occupational Therapy Manuscript submissions are welcome within any of the
will publish a special issue in 2016 on the topic of ‘Dimensions article categories listed in the Author’s Guide. Priority will
of dementia: the unique contribution of occupational therapy’. be given to manuscripts that will have a direct impact on
This special issue will provide an international forum for practice or policy. For further information see http://
research papers, critical reviews, practice analysis, and opinion www.cot.co.uk/contribute-and-submit-bjot/submit-bjot-
pieces relevant to theory, practice, research, education, and articles-online.
management related to occupational therapy’s contribution to Manuscripts should be submitted in the normal manner
dementia care. We are specifically looking for articles that via http://mc.manuscriptcentral.com/bjot and will undergo
explore the unique skill mix of occupational therapy as assessed peer review. Authors should indicate clearly in their cover-
by empirical research, and articles that address the different ing letter and at the end of the abstract that they wish their
dimensions of the experience of dementia. submission to be considered for inclusion in the ‘Dimensions
The special issue will be guest edited by Jackie Pool, of dementia’ special issue.
CEO of Jackie Pool Associates Ltd, and Dr Lesley Collier, The deadline for submissions is 24 November 2014.
Senior Lecturer in Occupational Therapy at the University Please send any enquiries in the first instance to: Dr
of Southampton and a member of the British Journal of Katharine Norman, Editor, email: katharine.noman@cot.co.uk,
Occupational Therapy’s Editorial Board. Tel: +44 (0)20 7450 2338.
380 British Journal of Occupational Therapy July 2014 77(7)
Downloaded from bjo.sagepub.com at KAI NAN UNIV on March 3, 2015
You might also like
- Hubungan Stress Dan ImunDocument6 pagesHubungan Stress Dan ImunmegaNo ratings yet
- Ni Hms 383186Document8 pagesNi Hms 383186Yaniatul AfdaNo ratings yet
- NIH Public Access: Fatigue in Systemic Lupus ErythematosusDocument17 pagesNIH Public Access: Fatigue in Systemic Lupus ErythematosusYaniatul AfdaNo ratings yet
- TCRM 56063 Optimal Management of Fatigue in Patients With Systemic Lupu 100114Document12 pagesTCRM 56063 Optimal Management of Fatigue in Patients With Systemic Lupu 100114Yaniatul AfdaNo ratings yet
- NIH Public Access: Fatigue in Systemic Lupus ErythematosusDocument17 pagesNIH Public Access: Fatigue in Systemic Lupus ErythematosusYaniatul AfdaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Semana 23 - InglésDocument6 pagesSemana 23 - InglésMirella MeloNo ratings yet
- Middlemarch Realism and Symbolic Form AnalysisDocument31 pagesMiddlemarch Realism and Symbolic Form AnalysisprankiplayspranksNo ratings yet
- Drowning Slim Jim 1Document5 pagesDrowning Slim Jim 1Gary O'NeillNo ratings yet
- Discipline and Ideas in Applied SciencesDocument21 pagesDiscipline and Ideas in Applied SciencesFranklyn TroncoNo ratings yet
- Cindy Strange vs. Town of NolensvilleDocument20 pagesCindy Strange vs. Town of NolensvilleUSA TODAY NetworkNo ratings yet
- Public Safety Assessment ReportDocument3 pagesPublic Safety Assessment ReportElizaNo ratings yet
- Love in The Time of AlgorithmsDocument1 pageLove in The Time of AlgorithmsMy Nguyễn Thị DiễmNo ratings yet
- EED02 Notes1Document8 pagesEED02 Notes1Lem Merob100% (1)
- Tutorial 2 ExcerciseDocument5 pagesTutorial 2 ExcerciseThảo BùiNo ratings yet
- Natalia 27 (1997) CompleteDocument131 pagesNatalia 27 (1997) CompletePeter CroeserNo ratings yet
- ATP - Art. 1404-1457Document7 pagesATP - Art. 1404-1457Migoy DANo ratings yet
- Eng Lab ReportDocument22 pagesEng Lab ReportSHAIK UMAR FAROOQNo ratings yet
- Little Ready enDocument25 pagesLittle Ready enaaas a100% (1)
- Process Speech OutlineDocument1 pageProcess Speech OutlinesclarkgwNo ratings yet
- The Nature Notes of An Edwardian Lady (Holden, Edith) (Z-Library)Document200 pagesThe Nature Notes of An Edwardian Lady (Holden, Edith) (Z-Library)Victoria OyarzunNo ratings yet
- Faith in God's Control Over NatureDocument11 pagesFaith in God's Control Over NatureBoenYatorNo ratings yet
- Erosion Corrosion ReportDocument16 pagesErosion Corrosion ReportHamza Al MahanaNo ratings yet
- Philippine Supreme Court JurisprudenceDocument3 pagesPhilippine Supreme Court JurisprudenceNigel GarciaNo ratings yet
- Inquiry Based Lesson PlanDocument8 pagesInquiry Based Lesson Planapi-295760565100% (2)
- Statistics For MGMT I & IIDocument161 pagesStatistics For MGMT I & IIewnetuNo ratings yet
- Test-Paper No. 7 For The 8th C" - Form Teacher: Rodica Capița Student's Name - Știrbu Daniel - Date: 21 21 May.Document2 pagesTest-Paper No. 7 For The 8th C" - Form Teacher: Rodica Capița Student's Name - Știrbu Daniel - Date: 21 21 May.daniel100% (1)
- Sermon On The Choice of Food - Zwingli (1522)Document24 pagesSermon On The Choice of Food - Zwingli (1522)Jim West100% (2)
- Reflexive Pronoun: Object SubjectDocument5 pagesReflexive Pronoun: Object SubjectSiti Sarah Abdullah100% (1)
- Amir Ibn Abdullah Ibn Jarrah Al Quraisyi Al Fihri Al Makki Is One of The Group AsDocument2 pagesAmir Ibn Abdullah Ibn Jarrah Al Quraisyi Al Fihri Al Makki Is One of The Group AsNurhusnida TanjungNo ratings yet
- A. FRANCISCO REALTY v. CA AND SPS. ROMULO S.A. JAVILLONAR AND ERLINDA P. JAVILLONARDocument10 pagesA. FRANCISCO REALTY v. CA AND SPS. ROMULO S.A. JAVILLONAR AND ERLINDA P. JAVILLONARkhate alonzoNo ratings yet
- Anal IntercourseDocument16 pagesAnal Intercourseagustin cassinoNo ratings yet
- Kar Asia Vs CoronaDocument2 pagesKar Asia Vs CoronaMavic MoralesNo ratings yet
- 1.1.10 Practice - Complete Your Assignment (Practice)Document5 pages1.1.10 Practice - Complete Your Assignment (Practice)FizzlesNo ratings yet
- TESDA Advanced Housekeeping Course DesignDocument160 pagesTESDA Advanced Housekeeping Course Designjazzy mallariNo ratings yet
- Betty J Ackley - Gail B Ludwig - Nursing Diagnosis Handbook - An Evidence-Based Guide To Planning CareDocument1,553 pagesBetty J Ackley - Gail B Ludwig - Nursing Diagnosis Handbook - An Evidence-Based Guide To Planning CarePatrick Anani Etoughe80% (10)