You might also like
- Kidney Transplant Management: A Guide to Evaluation and ComorbiditiesFrom EverandKidney Transplant Management: A Guide to Evaluation and ComorbiditiesNo ratings yet
- A Retrospective Cohort Study On The Clinical Outcomes of Patients Admitted To Intensive Care Units With DysnatremiaDocument10 pagesA Retrospective Cohort Study On The Clinical Outcomes of Patients Admitted To Intensive Care Units With DysnatremiaEdo RezaprasgaNo ratings yet
- Emergency Department Length of Stay and Mortality in Critically Injured Patients (2021)Document10 pagesEmergency Department Length of Stay and Mortality in Critically Injured Patients (2021)Kenmaster WirelessNo ratings yet
- Harris 2012Document5 pagesHarris 2012Nurul AidaNo ratings yet
- George-2020-Sedation Depth Is Associated WithDocument18 pagesGeorge-2020-Sedation Depth Is Associated WithDereje BayissaNo ratings yet
- Biomedical Journal: SciencedirectDocument6 pagesBiomedical Journal: SciencedirectFarihah SamarraNo ratings yet
- Intermediate Care Units and Their Role in Medical WardsDocument2 pagesIntermediate Care Units and Their Role in Medical WardsJHNo ratings yet
- Jocs 14583Document4 pagesJocs 14583Geysel SuarezNo ratings yet
- NIH Public Access: Predictors of Clinical Outcome After Tracheotomy in Critically Ill Obese PatientsDocument9 pagesNIH Public Access: Predictors of Clinical Outcome After Tracheotomy in Critically Ill Obese PatientsNaye Gmen DezNo ratings yet
- Documento PDFDocument7 pagesDocumento PDFMaría Fernanda Venegas CuevasNo ratings yet
- Endocarditis in The Intensive Care Unit An UpdateDocument10 pagesEndocarditis in The Intensive Care Unit An Updatecarper454No ratings yet
- Chen 2017Document7 pagesChen 2017Miranti Dea DoraNo ratings yet
- NAC Hospi UCI y SalasDocument10 pagesNAC Hospi UCI y Salasgiseladelarosa2006No ratings yet
- Achieving Sustainability in Reducing Unplanned Extubations in PICUDocument7 pagesAchieving Sustainability in Reducing Unplanned Extubations in PICUKevin Bazán TorrealvaNo ratings yet
- The Impact of Opening A Medical Step-Down Unit On Medically Critically Ill Patient Outcomes and Throughput - A Difference-in-Differences AnalysisDocument13 pagesThe Impact of Opening A Medical Step-Down Unit On Medically Critically Ill Patient Outcomes and Throughput - A Difference-in-Differences AnalysisJHNo ratings yet
- Epidemiology and Outcomes of Infectious SpondylodiDocument24 pagesEpidemiology and Outcomes of Infectious SpondylodiYogesh MVNo ratings yet
- 加拿大食道癌Document8 pages加拿大食道癌Joseph ChenNo ratings yet
- Outcome of Patients Undergoing Prolonged Mechanical Ventilation (Crit Care Med 2007)Document7 pagesOutcome of Patients Undergoing Prolonged Mechanical Ventilation (Crit Care Med 2007)alexgonzalezherNo ratings yet
- 1 s2.0 S1053077022009168 MainDocument8 pages1 s2.0 S1053077022009168 MainOttofianus Alvedo Hewick KalangiNo ratings yet
- Complication and Revision Rates Following Total Elbow Arthroplasty JHS Am 2011Document6 pagesComplication and Revision Rates Following Total Elbow Arthroplasty JHS Am 2011JT DanielsNo ratings yet
- 4.NIKEN-crowding Destinaion PDFDocument7 pages4.NIKEN-crowding Destinaion PDFAli Akbar RahmaniNo ratings yet
- Swift 2Document1 pageSwift 2Innani Wildania HusnaNo ratings yet
- Evolving Trends in Infective Endocarditis in A Developing Country: A Consequence of Medical Progress?Document9 pagesEvolving Trends in Infective Endocarditis in A Developing Country: A Consequence of Medical Progress?Hassan Abdi JamaNo ratings yet
- AnestesiDocument7 pagesAnestesiAnonymous yfIFkVUANo ratings yet
- Epidemiology, Risk Profile, Management, and Outcome in Geriatric Patients With Atrial Fibrillation in Two Long Term Care HospitalsDocument9 pagesEpidemiology, Risk Profile, Management, and Outcome in Geriatric Patients With Atrial Fibrillation in Two Long Term Care HospitalsGrupo A Medicina UAEMNo ratings yet
- IPHMILitRev V5.2Document5 pagesIPHMILitRev V5.2miguel angel camachoNo ratings yet
- ICU Registered Nurses 2Document8 pagesICU Registered Nurses 211 - JEMELYN LOTERTENo ratings yet
- Readmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsDocument9 pagesReadmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsbobNo ratings yet
- 2017 Article 133Document8 pages2017 Article 133Sastra NopiNo ratings yet
- Critical Care Goals and ObjectivesDocument28 pagesCritical Care Goals and ObjectivesjyothiNo ratings yet
- 20 - 3016 Faraz MansoorDocument5 pages20 - 3016 Faraz MansoorAwais ChatthaNo ratings yet
- Emergency Department Based Monoclonal Antibody TheDocument2 pagesEmergency Department Based Monoclonal Antibody The88fqjgsdk5No ratings yet
- 1041 4798 1 PBDocument5 pages1041 4798 1 PBBeti KristinawatiNo ratings yet
- Sharshar 2009 Debil y EstadiaDocument7 pagesSharshar 2009 Debil y EstadiaStefania Anahi MartelNo ratings yet
- 1471 2377 12 13 PDFDocument6 pages1471 2377 12 13 PDFSambit DashNo ratings yet
- HHS Public AccessDocument14 pagesHHS Public AccessPepe OcaNo ratings yet
- Intruduccion 1Document9 pagesIntruduccion 1BLANCA TATIANA PONCIANO MERINONo ratings yet
- Background of The StudyDocument6 pagesBackground of The StudyDan Kenneth Liban LlantoNo ratings yet
- 30 54 1 SMDocument7 pages30 54 1 SMNYONGKERNo ratings yet
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsDocument9 pagesResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998No ratings yet
- Lung Protective VentilationDocument28 pagesLung Protective VentilationJesus FrancoNo ratings yet
- Distress PosquirurgicoDocument18 pagesDistress PosquirurgicoMelina AlcaineNo ratings yet
- Extubacion NocturnaDocument29 pagesExtubacion NocturnaGustavoGarcíaNo ratings yet
- Art:10.1186/s13054 016 1252 2Document9 pagesArt:10.1186/s13054 016 1252 2IsnaNo ratings yet
- BEDsoresDocument9 pagesBEDsoresGeoffrey KimaniNo ratings yet
- Short and Long-Term Outcomes After Surgical Procedures Lasting For More Than Six HoursDocument8 pagesShort and Long-Term Outcomes After Surgical Procedures Lasting For More Than Six HoursDickyNo ratings yet
- s41598 021 88207 6 PDFDocument8 pagess41598 021 88207 6 PDFManuel ArenasNo ratings yet
- JCM 11 03457Document8 pagesJCM 11 03457Dania De la CruzNo ratings yet
- Journal Pone 0224563Document13 pagesJournal Pone 0224563Jhony FloresNo ratings yet
- Chest EgdtDocument6 pagesChest EgdtDhanny AdhityaNo ratings yet
- International Journal of Cardiology: SciencedirectDocument6 pagesInternational Journal of Cardiology: SciencedirectRobsonBorgesNo ratings yet
- ABCDEF Critical CareDocument19 pagesABCDEF Critical CarealbaNo ratings yet
- The Effect of An Emergency Department Dedicated Midtrack Area On Patient FlowDocument6 pagesThe Effect of An Emergency Department Dedicated Midtrack Area On Patient FlowBeny HermawanNo ratings yet
- Er ReadingsDocument6 pagesEr ReadingsReginald UyNo ratings yet
- The Perioperative Complication Rate of Orthopedic PDFDocument10 pagesThe Perioperative Complication Rate of Orthopedic PDFAnh Nguyen HuuNo ratings yet
- Incidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorDocument6 pagesIncidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorTomasNo ratings yet
- 3 DC 3Document8 pages3 DC 3astutikNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofAram Dumnoen-ngamNo ratings yet
- Jurnal LainDocument22 pagesJurnal LainBudi ArsanaNo ratings yet
- Aborto Septico Lanari-USA ICM 2004Document6 pagesAborto Septico Lanari-USA ICM 2004pastorizaariana25No ratings yet
- UntitledDocument45 pagesUntitledjemNo ratings yet
- Unit 2: TransducerDocument24 pagesUnit 2: TransducerROYAL GAMER YTNo ratings yet
- Combustion FundamentalsDocument30 pagesCombustion FundamentalsPrem SagarNo ratings yet
- LoperAmid 1Document5 pagesLoperAmid 1Hemma KusumaningrumNo ratings yet
- Lecture 4 EMADocument36 pagesLecture 4 EMAYai IbrahimNo ratings yet
- Future Scope and ConclusionDocument13 pagesFuture Scope and ConclusionGourab PalNo ratings yet
- University of Dar Es Salaam: Faculty of Commerce and ManagementDocument37 pagesUniversity of Dar Es Salaam: Faculty of Commerce and ManagementEric MitegoNo ratings yet
- Admission Prspectus English 2021-2022Document9 pagesAdmission Prspectus English 2021-2022A.B. SiNo ratings yet
- Archaeology - October 2016 PDFDocument72 pagesArchaeology - October 2016 PDFOmer CetinkayaNo ratings yet
- D6 Gamemasters Aid Screen Weg51019eOGLDocument40 pagesD6 Gamemasters Aid Screen Weg51019eOGLMr DM100% (1)
- Net June 2013Document22 pagesNet June 2013Sunil PandeyNo ratings yet
- CNL DivisionDocument38 pagesCNL DivisionaniketnareNo ratings yet
- Research Proposal Sample OutlineDocument17 pagesResearch Proposal Sample OutlineGuidance and Counseling OfficeNo ratings yet
- Engine Interface ModuleDocument3 pagesEngine Interface ModuleLuciano Pereira0% (2)
- Glorious Mysteries 1Document5 pagesGlorious Mysteries 1Vincent safariNo ratings yet
- Number SystemsDocument25 pagesNumber SystemsMehwish BilalNo ratings yet
- Body LanguageDocument17 pagesBody LanguageAR PiZaNo ratings yet
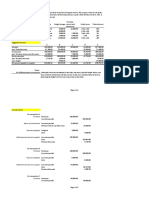
- Handout No. 03 - Purchase TransactionsDocument4 pagesHandout No. 03 - Purchase TransactionsApril SasamNo ratings yet
- Sculpture and ArchitectureDocument9 pagesSculpture and ArchitectureIngrid Dianne Luga BernilNo ratings yet
- Elaborare Modele de Rating in Conformitate Cu IFRS 9Document8 pagesElaborare Modele de Rating in Conformitate Cu IFRS 9MstefNo ratings yet
- Purchase Spec. For Bar (SB425)Document4 pagesPurchase Spec. For Bar (SB425)Daison PaulNo ratings yet
- Entropy (Information Theory)Document17 pagesEntropy (Information Theory)joseph676No ratings yet
- Estimation of Measurement Uncertainty For Electrical Conductivity in WaterDocument4 pagesEstimation of Measurement Uncertainty For Electrical Conductivity in WaterMaruthi KNo ratings yet
- The Future of Comparative Literary StudiesDocument14 pagesThe Future of Comparative Literary StudiesNabeesath ArifaNo ratings yet
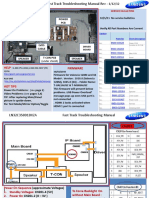
- Samsung LN55C610N1FXZA Fast Track Guide (SM)Document4 pagesSamsung LN55C610N1FXZA Fast Track Guide (SM)Carlos OdilonNo ratings yet
- The Effect of Realistic Mathematics Education Approach On Students' Achievement and Attitudes Towards MathematicsDocument9 pagesThe Effect of Realistic Mathematics Education Approach On Students' Achievement and Attitudes Towards MathematicsyusfazilaNo ratings yet
- Pengaruh Promosi Dan Brand Image (Citra Produk) Terhadap Loyalitas Pembelian Produk Pepsodent Di Ramayana Plaza, Jalan Aksara, Medan Dita AmanahDocument13 pagesPengaruh Promosi Dan Brand Image (Citra Produk) Terhadap Loyalitas Pembelian Produk Pepsodent Di Ramayana Plaza, Jalan Aksara, Medan Dita AmanahAhmad HerdandiNo ratings yet
- Simon Bolivar PresentationDocument7 pagesSimon Bolivar Presentationapi-345742212No ratings yet
- Another Look at Pistis ChristouDocument17 pagesAnother Look at Pistis Christouakimel100% (1)
- Blaine Ray HandoutDocument24 pagesBlaine Ray Handoutaquilesanchez100% (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (28)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (393)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (4)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)