You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Ballard ScoreDocument1 pageBallard ScoreFikriyah FuadiyahNo ratings yet
- Physiology Introduction and PrinciplesDocument81 pagesPhysiology Introduction and PrinciplesDeomicah SolanoNo ratings yet
- GPC RPM Pretermino Rcog 2019Document15 pagesGPC RPM Pretermino Rcog 2019Benjamin Miranda ValentinNo ratings yet
- 2017 Stroke in Childhood - Pathway PosterDocument1 page2017 Stroke in Childhood - Pathway PosterDeomicah SolanoNo ratings yet
- ABG SamplingDocument4 pagesABG SamplingDeomicah SolanoNo ratings yet
- Dengue in Children 2017Document18 pagesDengue in Children 2017Deomicah SolanoNo ratings yet
- Pediatric Measles Diagnosis and TreatmentDocument20 pagesPediatric Measles Diagnosis and TreatmentDeomicah SolanoNo ratings yet
- Physiology Finals ReviewerDocument22 pagesPhysiology Finals ReviewerDeomicah SolanoNo ratings yet
- Aplastic Anemia: Deomicah D. SolanoDocument17 pagesAplastic Anemia: Deomicah D. SolanoDeomicah SolanoNo ratings yet
- 2 Comparison of Maternal CRP With WBC Count in Predicting Intra Amniotic Infection in Premature Rupture of MembranesDocument4 pages2 Comparison of Maternal CRP With WBC Count in Predicting Intra Amniotic Infection in Premature Rupture of MembranesDeomicah SolanoNo ratings yet
- Neurology 1.02 The Neurological Examination - Dr. PunsalanDocument4 pagesNeurology 1.02 The Neurological Examination - Dr. PunsalanDeomicah SolanoNo ratings yet
- Neurology I: Approach to Cerebral FunctionDocument7 pagesNeurology I: Approach to Cerebral FunctionDeomicah SolanoNo ratings yet
- ABG Sampling (10-15 SOLANO) .OdtDocument4 pagesABG Sampling (10-15 SOLANO) .OdtDeomicah SolanoNo ratings yet
- ABG Sampling (10-15 SOLANO) .OdtDocument4 pagesABG Sampling (10-15 SOLANO) .OdtDeomicah SolanoNo ratings yet
- Surgery Systemic Response To Injury 1-9-2018Document67 pagesSurgery Systemic Response To Injury 1-9-2018Deomicah SolanoNo ratings yet
- Morning Endorsement: October 7, 2020 Group 10 - Subgroup 3Document26 pagesMorning Endorsement: October 7, 2020 Group 10 - Subgroup 3Deomicah SolanoNo ratings yet
- OINA Table PDFDocument16 pagesOINA Table PDFMichelle Joy Delos Reyes100% (1)
- Covid-19 On Pediatric Patients Part 1 (10-15 Solano)Document25 pagesCovid-19 On Pediatric Patients Part 1 (10-15 Solano)Deomicah SolanoNo ratings yet
- Gen. Path Lab4 PDFDocument100 pagesGen. Path Lab4 PDFDeomicah SolanoNo ratings yet
- Bacterial Identification and StrategiesDocument9 pagesBacterial Identification and StrategiesDeomicah Solano100% (1)
- Legal Medicine Solis NotesDocument9 pagesLegal Medicine Solis NotesDeomicah SolanoNo ratings yet
- RBC Morphology and InclusionsDocument3 pagesRBC Morphology and InclusionsDeomicah SolanoNo ratings yet
- Wound Healing PDFDocument46 pagesWound Healing PDFDeomicah SolanoNo ratings yet
- Hematology3 PDFDocument46 pagesHematology3 PDFDeomicah SolanoNo ratings yet
- Legal Medicine Solis NotesDocument100 pagesLegal Medicine Solis NotesMykee Naval88% (49)
- RBC&WBC AbnormalitiesDocument10 pagesRBC&WBC AbnormalitiesDeomicah SolanoNo ratings yet
- Wound Healing PDFDocument46 pagesWound Healing PDFDeomicah SolanoNo ratings yet
- Chest Trauma 2017 PDFDocument96 pagesChest Trauma 2017 PDFDeomicah SolanoNo ratings yet
- RBC and WBC Abnormalities in Blood SmearsDocument38 pagesRBC and WBC Abnormalities in Blood SmearsTorillo KimNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Complete blood count, CBC With Diff. and blood lm: B10845383 International Medical Center 20.5.2021 2:28 ًءﺎﺴﻣDocument6 pagesComplete blood count, CBC With Diff. and blood lm: B10845383 International Medical Center 20.5.2021 2:28 ًءﺎﺴﻣNizar AlharbiNo ratings yet
- C42135AA Beckman Coulter ClearLLab 10C Casebook PDFDocument586 pagesC42135AA Beckman Coulter ClearLLab 10C Casebook PDFHam Bone100% (1)
- Everything You Need to Know About Blood Composition and FunctionDocument31 pagesEverything You Need to Know About Blood Composition and FunctionHarshil PatelNo ratings yet
- Synevo Results 5Document3 pagesSynevo Results 5Kenan BagirNo ratings yet
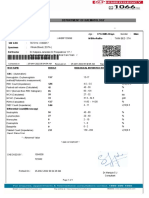
- Department of Haematology - : Mr. Nagaraja N 72yr 0Mth 3days Male Uhid Sin /LRN W/Bno/RefnoDocument1 pageDepartment of Haematology - : Mr. Nagaraja N 72yr 0Mth 3days Male Uhid Sin /LRN W/Bno/RefnoPrashanth NNo ratings yet
- RBC&WBC CountDocument29 pagesRBC&WBC CountShivangi ChandraNo ratings yet
- ADAPTIVE IMMUNITY (Rev - DR. Amoani)Document83 pagesADAPTIVE IMMUNITY (Rev - DR. Amoani)Boateng DerrickNo ratings yet
- Robbins Pathology - Chapter 6 TransDocument31 pagesRobbins Pathology - Chapter 6 Transnath nathNo ratings yet
- MojoDocument2 pagesMojokike1790No ratings yet
- Ana PhyDocument4 pagesAna PhyJustine Mae OyongNo ratings yet
- Cells Immune System Click Learn WorksheetDocument3 pagesCells Immune System Click Learn WorksheetRivera Cante DiegoNo ratings yet
- Children's FBC Reference RangesDocument1 pageChildren's FBC Reference RangesPat MobileNo ratings yet
- Hematology AtlasDocument733 pagesHematology Atlasrakshit09100% (10)
- CBC With DiffDocument2 pagesCBC With DiffLila AliNo ratings yet
- SNAB 7.18 Immunity FlashcardsDocument2 pagesSNAB 7.18 Immunity FlashcardsMeidayNo ratings yet
- Physio. D. Suroor. L1. BloodDocument24 pagesPhysio. D. Suroor. L1. Bloodزين العابدين محمد عويشNo ratings yet
- Heamtopoises ReviewerDocument17 pagesHeamtopoises ReviewerClyde BaltazarNo ratings yet
- Hemotology ReviewDocument61 pagesHemotology ReviewSukma EffendyNo ratings yet
- (MT 6318 LAB) Compiled 3rd Shifting TopicsDocument21 pages(MT 6318 LAB) Compiled 3rd Shifting Topicslanceferdinand.tan.pharmaNo ratings yet
- Degeneration and Regenration of Nerve Fibers by Dr. RoomiDocument11 pagesDegeneration and Regenration of Nerve Fibers by Dr. RoomiMudassar RoomiNo ratings yet
- Rehman Medical Institute: Test Result Unit Reference ValuesDocument1 pageRehman Medical Institute: Test Result Unit Reference ValuesfahadbasahirNo ratings yet
- Pathophysiology of Graft Versus Host DiseaseDocument2 pagesPathophysiology of Graft Versus Host DiseasePriMaNo ratings yet
- WBCs 1Document21 pagesWBCs 1kandarpvyasa5930No ratings yet
- Childrens FBC Reference Ranges PDFDocument1 pageChildrens FBC Reference Ranges PDFWarisatul Imam LubisNo ratings yet
- MLT MCQDocument13 pagesMLT MCQRamesh Rangu88% (8)
- Baby UZMA's Complete Haemogram ReportDocument2 pagesBaby UZMA's Complete Haemogram ReportmonsterindiaNo ratings yet
- GranulocitopoezaDocument34 pagesGranulocitopoezaNona NonicaNo ratings yet
- DgReportingVF PDFDocument2 pagesDgReportingVF PDFRamani DantuluriNo ratings yet
- Bone Marrow, Blood, Formation, Med TechDocument47 pagesBone Marrow, Blood, Formation, Med TechAngela Louise SmithsNo ratings yet
- EZH1 iPSC CAR TDocument23 pagesEZH1 iPSC CAR T111No ratings yet