You might also like
- Nihms 227802 PDFDocument19 pagesNihms 227802 PDFAntoninus HengkyNo ratings yet
- The Bidirectional Relationship Between TuberculosiDocument7 pagesThe Bidirectional Relationship Between TuberculosiJunita Nelly Esther JosephNo ratings yet
- Bchen,+5304 Blinded+Manuscript 9290 1 10 20200331Document6 pagesBchen,+5304 Blinded+Manuscript 9290 1 10 20200331sofia cianiNo ratings yet
- The Double Burden of Diabetes and Global Infection in Low and Middle-Income CountriesDocument9 pagesThe Double Burden of Diabetes and Global Infection in Low and Middle-Income CountrieslatifakhumairNo ratings yet
- Chronic Liver Disease Epid 2021Document6 pagesChronic Liver Disease Epid 2021Adrian ssNo ratings yet
- Epidemiology of Diabetes MellitusDocument5 pagesEpidemiology of Diabetes Mellitusarkanthos77No ratings yet
- COVID-19 impact on diabetes careDocument3 pagesCOVID-19 impact on diabetes careAynun JMNo ratings yet
- Obesity and The Risk and Outcome of Infection 2013Document8 pagesObesity and The Risk and Outcome of Infection 2013Melvin RosalezNo ratings yet
- BR J Haematol - 2015 - Vishnu - Haematological Manifestations of Human Immune Deficiency Virus InfectionDocument15 pagesBR J Haematol - 2015 - Vishnu - Haematological Manifestations of Human Immune Deficiency Virus InfectionRogelio Alban RugelNo ratings yet
- Epidemiological and Nutrition Transition in Developing Countries: Impact On Human Health and DevelopmentDocument9 pagesEpidemiological and Nutrition Transition in Developing Countries: Impact On Human Health and DevelopmentariniNo ratings yet
- Glucose Abnormalities in Patients With Hepatitis C Virus InfectionDocument10 pagesGlucose Abnormalities in Patients With Hepatitis C Virus InfectionElena BivolNo ratings yet
- Il 6 New FullDocument13 pagesIl 6 New FullAnindhiani Aparamitha SariNo ratings yet
- Te Burden and RisksDocument15 pagesTe Burden and RisksAgustin StadlerNo ratings yet
- Epidemiology of Diabetes: Key PointsDocument8 pagesEpidemiology of Diabetes: Key PointsSinau RekNo ratings yet
- Etiology and Evaluation of Diarrhea in AIDS: A Global Perspective at The MillenniumDocument10 pagesEtiology and Evaluation of Diarrhea in AIDS: A Global Perspective at The MillenniumSri Nowo MinartiNo ratings yet
- Diabetes As A Risk Factor For Periodontal Disease, Plausible MechanismsDocument13 pagesDiabetes As A Risk Factor For Periodontal Disease, Plausible MechanismsNishtha KumarNo ratings yet
- HIV Infection Epidemiology, Pathogenesis, Treatment, and PreventionDocument14 pagesHIV Infection Epidemiology, Pathogenesis, Treatment, and PreventionandresgarciafNo ratings yet
- Atkinson 2014Document14 pagesAtkinson 2014nagitagtgtNo ratings yet
- Tuberculosis and Diabetes Mellitus - An Underappreciated AssociationDocument9 pagesTuberculosis and Diabetes Mellitus - An Underappreciated AssociationNajla rayNo ratings yet
- Anemia As A Prognostic Marker For Disease Progression in HIV InfectionDocument12 pagesAnemia As A Prognostic Marker For Disease Progression in HIV InfectionKIU PUBLICATION AND EXTENSIONNo ratings yet
- Hodgson 2015Document15 pagesHodgson 2015gunawanNo ratings yet
- HIV/AIDS: A Guide to the Virus and Its Disease StatesDocument7 pagesHIV/AIDS: A Guide to the Virus and Its Disease StatesWeny NoralitaNo ratings yet
- The Association of Obesity and Severe Dengue - Possible PathophysiologicaDocument14 pagesThe Association of Obesity and Severe Dengue - Possible PathophysiologicaTaufiqurrokhman RofiiNo ratings yet
- HHS Public AccessDocument19 pagesHHS Public AccessIvan DanindraNo ratings yet
- Periodontal Infection and Glycemic Control in Diabetes: Current EvidenceDocument5 pagesPeriodontal Infection and Glycemic Control in Diabetes: Current EvidencegarciamanuelNo ratings yet
- Risk Factors for Poor TB Outcomes (38 charactersDocument3 pagesRisk Factors for Poor TB Outcomes (38 charactersALRpwjNo ratings yet
- Hepatitis C in PregnancyDocument9 pagesHepatitis C in PregnancychanyundaNo ratings yet
- Hepa Changes in ManagementDocument9 pagesHepa Changes in Managemente.foresgilNo ratings yet
- Epidemiologyand Pathogenesisofulcerative Colitis: Lillian Du,, Christina HaDocument12 pagesEpidemiologyand Pathogenesisofulcerative Colitis: Lillian Du,, Christina HaVinicius BalanNo ratings yet
- Trujillo-Ochoa2018 Hav in MexicoDocument9 pagesTrujillo-Ochoa2018 Hav in MexicoOliver Viera SeguraNo ratings yet
- Resume Jurnal AKLDocument8 pagesResume Jurnal AKLLenggogeni HumairaNo ratings yet
- HIV Disease and NutritionDocument10 pagesHIV Disease and Nutritionmariosan81No ratings yet
- Tuverculosis in OlderDocument13 pagesTuverculosis in OlderjcarloscangalayaNo ratings yet
- 1 s2.0 S0953620522002151 MainDocument6 pages1 s2.0 S0953620522002151 MainErika WulandariNo ratings yet
- Tuberculosis and HIV Infection: The Global Setting: SupplementarticleDocument10 pagesTuberculosis and HIV Infection: The Global Setting: SupplementarticleCaster BondoNo ratings yet
- Naskah Publikasi (Ali)Document11 pagesNaskah Publikasi (Ali)Eka Nurul SIamNo ratings yet
- Ditorial: Type 2 Diabetes Mellitus and Its Complications: From The Mo-Lecular Biology To The Clinical PracticeDocument4 pagesDitorial: Type 2 Diabetes Mellitus and Its Complications: From The Mo-Lecular Biology To The Clinical PracticePugi KurbyNo ratings yet
- Hepatitis A-PrintDocument17 pagesHepatitis A-PrintVirginia EchoNo ratings yet
- TB Burden Qatar: (CITATION Abu18 /L 1033)Document10 pagesTB Burden Qatar: (CITATION Abu18 /L 1033)Ahmad HashmiNo ratings yet
- حنينDocument12 pagesحنينHanen sayar AlmarshedyةNo ratings yet
- Type 2 Diabetes: Annals of Internal MedicineDocument16 pagesType 2 Diabetes: Annals of Internal MedicineLAURA AGUILAR ARANGONo ratings yet
- Exploring The Risk of SevereDocument3 pagesExploring The Risk of Severexc_corinaNo ratings yet
- Epidemiology - Diabetes and Kidney Disease PDFDocument12 pagesEpidemiology - Diabetes and Kidney Disease PDFSharyna EmyraNo ratings yet
- HIV Resistance in Patients With Sickle Cell AnaemiaDocument3 pagesHIV Resistance in Patients With Sickle Cell AnaemiaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Research Proposal Final DraftDocument110 pagesResearch Proposal Final Draftapi-549811354No ratings yet
- Sim2021 Article GastrointestinalDysfunctionAndDocument6 pagesSim2021 Article GastrointestinalDysfunctionAndVadNo ratings yet
- Bdb06ff135c7ccb File 2Document29 pagesBdb06ff135c7ccb File 2Mary ThaherNo ratings yet
- Prevalence Diabetes ObesityDocument14 pagesPrevalence Diabetes ObesityNasrin SharifiNo ratings yet
- 10 1111@hel 12741Document8 pages10 1111@hel 12741Catalina ChNo ratings yet
- HIV Infection and Cardiovascular Diseases The Obnoxious DuosDocument5 pagesHIV Infection and Cardiovascular Diseases The Obnoxious DuosKIU PUBLICATION AND EXTENSIONNo ratings yet
- Orthodontic Considerations in The Diabetic Patient: Luc Bensch, Marc Braem, and Guy WillemsDocument7 pagesOrthodontic Considerations in The Diabetic Patient: Luc Bensch, Marc Braem, and Guy WillemsRanda KamelNo ratings yet
- Systemic 1Document10 pagesSystemic 1Prarthana PaiNo ratings yet
- 2022 EHGNA y DM Revision Cusi Lancet End 2022Document13 pages2022 EHGNA y DM Revision Cusi Lancet End 2022Everardo Josué Díaz LópezNo ratings yet
- Classification Pathophysiology Diagnosis and ManagDocument10 pagesClassification Pathophysiology Diagnosis and ManagHeru SetiawanNo ratings yet
- Estimates On HCV Disease Burden Worldwide - Filling The GapsDocument5 pagesEstimates On HCV Disease Burden Worldwide - Filling The GapsRobert G. Gish, MDNo ratings yet
- Periodontal disease in HIV/AIDS patientsDocument20 pagesPeriodontal disease in HIV/AIDS patientsANA VERONICA MAYORGA MORALESNo ratings yet
- Type 2 Diabetes: Annals of Internal MedicineDocument16 pagesType 2 Diabetes: Annals of Internal Medicineallele94No ratings yet
- Tuberculosis and HIV CoDocument34 pagesTuberculosis and HIV CoLouinel JosephNo ratings yet
- Campbell 2014 Anutoimmunity and The GutDocument12 pagesCampbell 2014 Anutoimmunity and The Gutdesign.your.life.1990No ratings yet
- No NPM Nama Mahasiswa Keteranga NDocument5 pagesNo NPM Nama Mahasiswa Keteranga NJordan FadhillaNo ratings yet
- Medikolegal - Pembagian Kelompok PBLDocument2 pagesMedikolegal - Pembagian Kelompok PBLJordan FadhillaNo ratings yet
- Conjunctivitis in COVID-19 PatientsDocument7 pagesConjunctivitis in COVID-19 PatientsStephanie AureliaNo ratings yet
- Medikolegal - Pembagian Kelompok PBLDocument2 pagesMedikolegal - Pembagian Kelompok PBLJordan FadhillaNo ratings yet
- 6362 Virtual Autopsy PDFDocument13 pages6362 Virtual Autopsy PDFnur annisyaNo ratings yet
- Bor Peserta Uas Blok Emergenci 2017 Selasa 11 Okt 2021Document4 pagesBor Peserta Uas Blok Emergenci 2017 Selasa 11 Okt 2021Jordan FadhillaNo ratings yet
- Bor Peserta Uas Blok Emergenci 2017 Selasa 11 Okt 2021Document4 pagesBor Peserta Uas Blok Emergenci 2017 Selasa 11 Okt 2021Jordan FadhillaNo ratings yet
- No NPM Nama Mahasiswa Keteranga NDocument5 pagesNo NPM Nama Mahasiswa Keteranga NJordan FadhillaNo ratings yet
- Assessment of Pharmacy Students' Clinical Skills Using Objective Structured Clinical Examination - A Literature ReviewDocument6 pagesAssessment of Pharmacy Students' Clinical Skills Using Objective Structured Clinical Examination - A Literature ReviewJordan FadhillaNo ratings yet
- 2726 PDF PDFDocument5 pages2726 PDF PDFJordan FadhillaNo ratings yet
- Students' Perception of Effect On Basic Clinical Skills Training in Preclinical Phase To National OSCEDocument8 pagesStudents' Perception of Effect On Basic Clinical Skills Training in Preclinical Phase To National OSCEJordan FadhillaNo ratings yet
- Medical Education: Assessment Clinical Using Objective Structured ExaminationDocument5 pagesMedical Education: Assessment Clinical Using Objective Structured ExaminationJordan FadhillaNo ratings yet
- 2726 PDF PDFDocument5 pages2726 PDF PDFJordan FadhillaNo ratings yet
- Objective Structure Clinical Examination (OSCE) Based Teaching Material DevelopmentDocument5 pagesObjective Structure Clinical Examination (OSCE) Based Teaching Material DevelopmentJordan FadhillaNo ratings yet
- 139 2009 BrandDocument7 pages139 2009 BrandJordan FadhillaNo ratings yet
- Students' Perception of Effect On Basic Clinical Skills Training in Preclinical Phase To National OSCEDocument8 pagesStudents' Perception of Effect On Basic Clinical Skills Training in Preclinical Phase To National OSCEJordan FadhillaNo ratings yet
- PICO - Indah S. Widyahening PDFDocument39 pagesPICO - Indah S. Widyahening PDFJordan FadhillaNo ratings yet
- Jadwal Blok Cardio FK Yarsi 2016/2017Document6 pagesJadwal Blok Cardio FK Yarsi 2016/2017Jordan FadhillaNo ratings yet
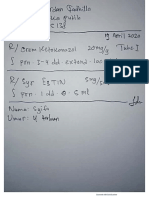
- Ujian Resep Online Yarsi 4Document1 pageUjian Resep Online Yarsi 4Jordan FadhillaNo ratings yet
- Ujian Resep Online Yarsi 2Document1 pageUjian Resep Online Yarsi 2Jordan FadhillaNo ratings yet
- PICO - Indah S. Widyahening PDFDocument39 pagesPICO - Indah S. Widyahening PDFJordan FadhillaNo ratings yet
- Cover Skenario 3 Blog Kardio - 2Document2 pagesCover Skenario 3 Blog Kardio - 2Jordan FadhillaNo ratings yet
- Presentasi MutasiDocument33 pagesPresentasi MutasimilatiNo ratings yet
- 139 2009 BrandDocument7 pages139 2009 BrandJordan FadhillaNo ratings yet
- Ujian Resep Online Yarsi 1Document1 pageUjian Resep Online Yarsi 1Jordan FadhillaNo ratings yet
- Zwasta Pribadi Mahardhika Key FindingsDocument24 pagesZwasta Pribadi Mahardhika Key FindingsMuhamad Ghifari AzharNo ratings yet
- Proteinuria Pada Anak AnakDocument7 pagesProteinuria Pada Anak Anaklathifa nabilaNo ratings yet
- ELYSION Virtual Region - 003 - CerulDocument363 pagesELYSION Virtual Region - 003 - CerulJordan FadhillaNo ratings yet
- Jadwal Blok Cardio FK Yarsi 2016/2017Document6 pagesJadwal Blok Cardio FK Yarsi 2016/2017Jordan FadhillaNo ratings yet
- Fever Proforma and Assignment - 1Document48 pagesFever Proforma and Assignment - 1SivaNo ratings yet
- PCV Septia 2003Document16 pagesPCV Septia 2003WondaNo ratings yet
- PEPTIC ULCER LESSON PLANDocument7 pagesPEPTIC ULCER LESSON PLANVeenasravanthiNo ratings yet
- Postural DrainageDocument6 pagesPostural DrainageKit Alizon Barredo0% (1)
- Articulo DermatitisDocument4 pagesArticulo DermatitisBethNo ratings yet
- Cavitary Lung Diseases: A Clinical-Radiologic Algorithmic ApproachDocument23 pagesCavitary Lung Diseases: A Clinical-Radiologic Algorithmic ApproachjhordyafsNo ratings yet
- Draft List of MicroorganismsDocument36 pagesDraft List of MicroorganismsAngadNo ratings yet
- Vazyme Antigen Test BrochureDocument2 pagesVazyme Antigen Test BrochureEddy LeoNo ratings yet
- Accomplishment ReportDocument3 pagesAccomplishment ReportGiles DayaNo ratings yet
- Acute AbdomenDocument35 pagesAcute AbdomenRonit ChandNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsCharan SinghNo ratings yet
- Ent Osce 2008Document22 pagesEnt Osce 2008salamred100% (2)
- Does Gastroesophageal Reflux Predispose To Rhinosinusitis? Predispone El Reflujo Gastroesofagico A Rinosinusitis?Document31 pagesDoes Gastroesophageal Reflux Predispose To Rhinosinusitis? Predispone El Reflujo Gastroesofagico A Rinosinusitis?Victor EnachiNo ratings yet
- 60 IzovacDocument3 pages60 Izovacuzairch491No ratings yet
- COPARDocument7 pagesCOPARMar VinNo ratings yet
- Document from அகத்தியன் அகாடமிDocument4 pagesDocument from அகத்தியன் அகாடமிarunkumarNo ratings yet
- On Cardio Respiratory ExerciseDocument9 pagesOn Cardio Respiratory ExercisegomNo ratings yet
- Referat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Document14 pagesReferat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Ahmad Fari Arief LopaNo ratings yet
- Colon CancerDocument1 pageColon Cancerapi-518183280No ratings yet
- FAQs on Novel Coronavirus (2019-nCoVDocument32 pagesFAQs on Novel Coronavirus (2019-nCoVJasper Rex RamirezNo ratings yet
- Student Nurses' Community: NURSING CARE PLAN Neonatal SepsisDocument2 pagesStudent Nurses' Community: NURSING CARE PLAN Neonatal SepsisChristian Remetio100% (1)
- PRC Ple Review 021318Document301 pagesPRC Ple Review 021318Maria Cecilia Luz Romero67% (6)
- Community DentistryDocument5 pagesCommunity DentistryDenis BaftijariNo ratings yet
- Case Report模板Document18 pagesCase Report模板ChenNo ratings yet
- Revised-Chapter 6 Case Study BDocument2 pagesRevised-Chapter 6 Case Study BAngelica PerezNo ratings yet
- ED Management of Abused ChildDocument63 pagesED Management of Abused ChildRam Kirubakar ThangarajNo ratings yet
- NCCN Guideline RC v3 2022Document20 pagesNCCN Guideline RC v3 2022dony hendrawanNo ratings yet
- Microbiology & Helminths: Classification, Morphology and Life CyclesDocument58 pagesMicrobiology & Helminths: Classification, Morphology and Life CyclesChrisfenna MadihvolNo ratings yet
- A Guide To Your: COVID-19 VaccinationDocument8 pagesA Guide To Your: COVID-19 Vaccinationalinaluca30No ratings yet
- Presentation 5 The Infection Control Risk Assessment and PlanDocument24 pagesPresentation 5 The Infection Control Risk Assessment and PlanLany PasauNo ratings yet