You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Kisah Joko Tinggkir Versi Bahasa InggrisDocument2 pagesKisah Joko Tinggkir Versi Bahasa Inggrishero masterNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Dongeng Bhs Inggris-Mouse Deer and CrocodileDocument2 pagesDongeng Bhs Inggris-Mouse Deer and CrocodileEthamHadipudjanaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Fairy Tale GagakDocument2 pagesFairy Tale Gagakhero masterNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Myth About Daung SnakeDocument2 pagesMyth About Daung Snakehero masterNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Nama: M.Nur Khafiddin KLS: IXA NO: 17Document1 pageNama: M.Nur Khafiddin KLS: IXA NO: 17Junizar FannyNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Fairy Tale of Kalimantan Island Lumba-LumbaDocument5 pagesFairy Tale of Kalimantan Island Lumba-Lumbahero masterNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Nama: M.Nur Khafiddin KLS: IXA NO: 17Document1 pageNama: M.Nur Khafiddin KLS: IXA NO: 17Junizar FannyNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Keong MasDocument2 pagesKeong Mashero masterNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Storry Telling CinderellaDocument2 pagesStorry Telling CinderellaRinorsa Duane AgustaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Fairy Tale Roro JongrangDocument1 pageFairy Tale Roro Jongranghero masterNo ratings yet
- Little Red Hood Fairy TaleDocument3 pagesLittle Red Hood Fairy Talehero masterNo ratings yet
- Jaka Dan AlpabetDocument3 pagesJaka Dan Alpabethero masterNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Beauty and The BeastDocument4 pagesBeauty and The BeastIssnadewi Paramitha WiryaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Once Upon A Time A Very Poor Woodcutter Lived in A Tiny Cottage in The Forest With His Two ChildrenDocument7 pagesOnce Upon A Time A Very Poor Woodcutter Lived in A Tiny Cottage in The Forest With His Two Childrenbianca0% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Dongeng Timun Mas English - IndonesiaDocument2 pagesDongeng Timun Mas English - Indonesiahero masterNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Arjuna Mencari CintaDocument4 pagesArjuna Mencari CintaRama ArjanaNo ratings yet
- Management of Cyclic Vomiting Syndrome.15 PDFDocument5 pagesManagement of Cyclic Vomiting Syndrome.15 PDFhero masterNo ratings yet
- Beauty and The BeastDocument4 pagesBeauty and The BeastIssnadewi Paramitha WiryaNo ratings yet
- S - Relationships Among Allergic Rhinitis, Asthma, and Chronic RhinosinusitisDocument4 pagesS - Relationships Among Allergic Rhinitis, Asthma, and Chronic RhinosinusitisMuta MimahNo ratings yet
- Presentation SubheadingDocument2 pagesPresentation SubheadingDhila- Nailatul FadhilahNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Jurnal NeuroDocument30 pagesJurnal Neurohero masterNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Daftar Pustaka Kanker Ovarium EpithelialDocument1 pageDaftar Pustaka Kanker Ovarium Epithelialhero masterNo ratings yet
- Dry Eye DonkDocument9 pagesDry Eye Donkhero masterNo ratings yet
- Status Epilepticus, Refractory Status Epilepticus, and Super-Refractory Status EpilepticusDocument25 pagesStatus Epilepticus, Refractory Status Epilepticus, and Super-Refractory Status EpilepticusAlvaro EstupiñanNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Journal Baru NeurologiDocument10 pagesJournal Baru Neurologihero masterNo ratings yet
- Click To Edit Master Subtitle StyleDocument4 pagesClick To Edit Master Subtitle StyleWawanNo ratings yet
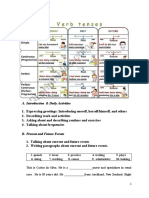
- Introducing Daily Activities and RoutinesDocument11 pagesIntroducing Daily Activities and RoutinesShafanaiNo ratings yet
- ETAT Ethiopia Manual For Participants May 20 2014 PRINTDocument184 pagesETAT Ethiopia Manual For Participants May 20 2014 PRINTNadik83% (6)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Case StudiesDocument5 pagesCase StudiesPou PunzalanNo ratings yet
- Circulation System in A Hospital 18 01 17Document44 pagesCirculation System in A Hospital 18 01 17Aaquib Mahfuz63% (8)
- Ancillary ServicesDocument88 pagesAncillary ServicesSangeeta BSR0% (1)
- ARD6P2 - G5 - GREGORIO Ritchell-Ann, LARIOSA Czarina Theresa, CUSTODIO Khate - POWERPOINT - PRESENTATIONDocument107 pagesARD6P2 - G5 - GREGORIO Ritchell-Ann, LARIOSA Czarina Theresa, CUSTODIO Khate - POWERPOINT - PRESENTATIONRitchelle Ann GregorioNo ratings yet
- Observation Care Evaluation and Management Codes PolicyDocument5 pagesObservation Care Evaluation and Management Codes PolicyAnonymous VrkWoC9No ratings yet
- Tahpi A To Z Brochure Jan 2017Document68 pagesTahpi A To Z Brochure Jan 2017api-264890887No ratings yet
- Hospitals PDFDocument30 pagesHospitals PDFBachir lejlifaNo ratings yet
- FSH Project Report ReviewDocument32 pagesFSH Project Report ReviewChan Nov0% (1)
- MGTS ZC211 (EC-3 Regular) First Semester 2019-2020 Page 1 of 2Document2 pagesMGTS ZC211 (EC-3 Regular) First Semester 2019-2020 Page 1 of 2balaji817150No ratings yet
- Project Plan Scenarios: HCS/412: Project Management For Health Care ProfessionalsDocument6 pagesProject Plan Scenarios: HCS/412: Project Management For Health Care ProfessionalsGlobal ComputerNo ratings yet
- Chest InjuryDocument3 pagesChest Injurysofia yapNo ratings yet
- Professional, Structural and Organisational Interventions in Primary Care For Reducing Medication ErrorsDocument147 pagesProfessional, Structural and Organisational Interventions in Primary Care For Reducing Medication ErrorsGurgehNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ishak Et Al, 2020Document16 pagesIshak Et Al, 2020widyadariNo ratings yet
- Trauma and Combat Critical Care in Clinical Practice - Sam DDocument539 pagesTrauma and Combat Critical Care in Clinical Practice - Sam DMotive FM 24 horas de Pura MotivaçãoNo ratings yet
- The Mobile Army Surgical Hospital (MASH) A Military and Surgical LegacyDocument9 pagesThe Mobile Army Surgical Hospital (MASH) A Military and Surgical LegacyHowardNo ratings yet
- Workplace ViolenceDocument80 pagesWorkplace Violencedustinkeener078573No ratings yet
- Medical Consent Form 25-6-15Document4 pagesMedical Consent Form 25-6-15Amogha KonammeNo ratings yet
- At The Hospital Quick Reference Glossary PDFDocument12 pagesAt The Hospital Quick Reference Glossary PDFFaisal IqbalNo ratings yet
- ER Nurse CVDocument5 pagesER Nurse CVLopezDistrict FarmersHospitalNo ratings yet
- VA Office of Inspector GeneralDocument46 pagesVA Office of Inspector Generalryan turbevilleNo ratings yet
- Common Medical AbbreviationsDocument10 pagesCommon Medical Abbreviationspg LNo ratings yet
- Santana Et Al How To Practice Person Centred CareDocument12 pagesSantana Et Al How To Practice Person Centred CareShita DewiNo ratings yet
- The Big Book of Accident PreventionDocument15 pagesThe Big Book of Accident PreventiontilahunNo ratings yet
- Post TestDocument11 pagesPost Testoomculun100% (6)
- Mental Health in ConnecticutDocument60 pagesMental Health in ConnecticutHelen BennettNo ratings yet
- Case StudiesDocument30 pagesCase Studiessiachen260% (1)
- After The Class Students Will Be Able To Gain Knowledge About TriageDocument3 pagesAfter The Class Students Will Be Able To Gain Knowledge About TriageRahul DamorNo ratings yet
- Imran Ahmad Sajid-Medical Social Work in Lady Reading Hospital, Peshawar, PakistanDocument52 pagesImran Ahmad Sajid-Medical Social Work in Lady Reading Hospital, Peshawar, PakistanimranahmadsajidNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)