You might also like
- Dr. Amy's Simplified Road Map To HealthDocument15 pagesDr. Amy's Simplified Road Map To HealthDr. Amy Yasko100% (46)
- Gel Electrophoresis Basics Worksheet: NameDocument2 pagesGel Electrophoresis Basics Worksheet: Nameapi-52265051475% (4)
- Data Interpretation For Medical StudentsDocument42 pagesData Interpretation For Medical StudentsPasTestBooks100% (6)
- Oral Surgery MCQDocument9 pagesOral Surgery MCQMohammed Qasim Al-Watary82% (11)
- Sideroblastic AnemiaDocument8 pagesSideroblastic AnemiaIslam Ahmady MohamedNo ratings yet
- USMLE - Heme & Lymph PathologyDocument21 pagesUSMLE - Heme & Lymph PathologyMatt McGlothlinNo ratings yet
- Math Contract PDFDocument129 pagesMath Contract PDFDanish Masood100% (1)
- Larynx Wrote by DR Nassem TalaatDocument38 pagesLarynx Wrote by DR Nassem TalaatAbouzr Mohammed ElsaidNo ratings yet
- A2 Biology Edexcel Textbook Answers To QuestionsDocument56 pagesA2 Biology Edexcel Textbook Answers To Questionsbulanula63% (19)
- Thrombosis Update: Simone M. Chang, Mercia Gondim, Michael HuangDocument3 pagesThrombosis Update: Simone M. Chang, Mercia Gondim, Michael HuangLunaNo ratings yet
- Differential Diagnosis of Microcytic Anemia PDFDocument5 pagesDifferential Diagnosis of Microcytic Anemia PDFayms99No ratings yet
- Cap 13Document88 pagesCap 13Saul RivasNo ratings yet
- Safety: Hemolytic HemorrhagicDocument6 pagesSafety: Hemolytic HemorrhagicAji Prima PutraNo ratings yet
- Hematologic DiseasesDocument19 pagesHematologic DiseasesismailcemNo ratings yet
- REVIEW Heart Failure in - Thalassemia Syndromes: A Decade of ProgressDocument11 pagesREVIEW Heart Failure in - Thalassemia Syndromes: A Decade of ProgressLuan MatosNo ratings yet
- Anemia of Chronic DiseaseDocument5 pagesAnemia of Chronic DiseaseGufront MustofaNo ratings yet
- Ncology UrseDocument16 pagesNcology Ursetricia_fernandoNo ratings yet
- Anemia DM-1 - REV.Document44 pagesAnemia DM-1 - REV.abdulrahmanbelewa96No ratings yet
- Utilizado - LiptonDocument9 pagesUtilizado - LiptondeliveryworkNo ratings yet
- SGL 2 (Hemolytic Anemia & Hemoglobinopathies)Document53 pagesSGL 2 (Hemolytic Anemia & Hemoglobinopathies)raman mahmudNo ratings yet
- Emergencymedicine Evaluationandmanagement Ofanemia: Brit Long,, Alex KoyfmanDocument22 pagesEmergencymedicine Evaluationandmanagement Ofanemia: Brit Long,, Alex KoyfmanVictor ChisNo ratings yet
- POSTER Trombosi CarotideaDocument1 pagePOSTER Trombosi CarotidearuoccoireneNo ratings yet
- Anaemia Management Whitepaper ENDocument8 pagesAnaemia Management Whitepaper ENNikhitha Mariya JohnNo ratings yet
- Joo Sten 2017Document7 pagesJoo Sten 2017langit rizki yuditamaNo ratings yet
- Chapter 14 - HematopathologyDocument66 pagesChapter 14 - Hematopathologynigel farageNo ratings yet
- Introduction To Anemia and ClassificationDocument10 pagesIntroduction To Anemia and ClassificationDarien LiewNo ratings yet
- An in-depth guide to evaluating and diagnosing anemiaDocument190 pagesAn in-depth guide to evaluating and diagnosing anemiaakbarNo ratings yet
- HEMATOLOGY Chapter 20 Rodaks Hematology, 5E (2016)Document14 pagesHEMATOLOGY Chapter 20 Rodaks Hematology, 5E (2016)Sachi Xandria de LaraNo ratings yet
- PallorDocument16 pagesPallorManal AlQuaimi100% (1)
- Anmia MicrociticaDocument8 pagesAnmia MicrociticafabitoxxpepeNo ratings yet
- Dental Considerations of Children With Anemias - An: Journal of Dentistry & Oral DisordersDocument6 pagesDental Considerations of Children With Anemias - An: Journal of Dentistry & Oral DisordersNindy PutriNo ratings yet
- Microcytic Anemia, Iron Deff Dan ThalasemiaDocument34 pagesMicrocytic Anemia, Iron Deff Dan ThalasemiaRoby KieranNo ratings yet
- Red Cell DisordersDocument38 pagesRed Cell DisordersMARTINEZ JUSTINENo ratings yet
- Red Blood Cell Morphology PDFDocument7 pagesRed Blood Cell Morphology PDFdianaNo ratings yet
- Cell AnemiaDocument12 pagesCell AnemiaAlejandra LópezNo ratings yet
- Besarab 2010Document13 pagesBesarab 2010josephNo ratings yet
- Microcytic Anemia PDFDocument8 pagesMicrocytic Anemia PDFMargarita TorresNo ratings yet
- Clinical - Aspects Diagnosis and Treatment of The Sideroblastic AnemiasDocument19 pagesClinical - Aspects Diagnosis and Treatment of The Sideroblastic AnemiasAnnel LozanoNo ratings yet
- RBC Alterations Link Diabetes and Alzheimer's DiseaseDocument10 pagesRBC Alterations Link Diabetes and Alzheimer's DiseasePutri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- 15 Sideroblastic AnemiaDocument24 pages15 Sideroblastic AnemiaKelvinTMaikanaNo ratings yet
- Leucemia Mieloide AgudaDocument43 pagesLeucemia Mieloide AgudaMichelle Mejia FamiliaNo ratings yet
- Anemia - AmbossDocument10 pagesAnemia - AmbossGuga XachidzeNo ratings yet
- Study Questions on Haematological DisordersDocument3 pagesStudy Questions on Haematological Disordersjess waldenNo ratings yet
- Pappenheimer Bodies: Lom-Oc, VillanuevaDocument16 pagesPappenheimer Bodies: Lom-Oc, VillanuevaSHUPATUSSAINo ratings yet
- Iron Defeciency AnemiaDocument7 pagesIron Defeciency AnemiaMaryam FadahNo ratings yet
- Rhabdomyolysis: A Review of The LiteratureDocument21 pagesRhabdomyolysis: A Review of The LiteratureMeicilia BahariNo ratings yet
- M.03 Hemolytic AnemiaDocument5 pagesM.03 Hemolytic AnemiaRaymund AldabaNo ratings yet
- RBC Disorder 2Document9 pagesRBC Disorder 2Dongho ShinNo ratings yet
- Case Report Pediatric Von&JepDocument23 pagesCase Report Pediatric Von&JepFarizan NurmushoffaNo ratings yet
- Red Blood Cells and Anaemias ClassificationDocument2 pagesRed Blood Cells and Anaemias ClassificationSubhasish BarikNo ratings yet
- Aplastic Anemia Is A NormocyticDocument17 pagesAplastic Anemia Is A NormocyticAfrio ArismanNo ratings yet
- Anaemia A Disease or SymptomDocument7 pagesAnaemia A Disease or SymptomJHEIBER ANTONIO HURTADO BEYTARNo ratings yet
- Dental Considerations in Thalassemic PatientsDocument6 pagesDental Considerations in Thalassemic PatientsInternational Organization of Scientific Research (IOSR)No ratings yet
- Sideroblastic Anemia Guide: Causes, Symptoms & TypesDocument18 pagesSideroblastic Anemia Guide: Causes, Symptoms & TypesSonam Joshi100% (2)
- HaematopathologyDocument253 pagesHaematopathologyamyNo ratings yet
- HaematologyDocument28 pagesHaematologyfh fgNo ratings yet
- Anemia PDFDocument6 pagesAnemia PDFMatthew GiscombeNo ratings yet
- Nejmct1004810 2Document11 pagesNejmct1004810 2fathia1805No ratings yet
- Anemia of Chronic DiseaseDocument2 pagesAnemia of Chronic DiseasejuanabNo ratings yet
- Anemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDocument15 pagesAnemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDanielle FosterNo ratings yet
- Thalassemia: An Inherited Blood DisorderDocument1 pageThalassemia: An Inherited Blood DisorderprinceamitNo ratings yet
- Aplastic Anemia - An Overview: DR Aniruddh Shrivastava Guided By: DR S.H. Talib SIRDocument42 pagesAplastic Anemia - An Overview: DR Aniruddh Shrivastava Guided By: DR S.H. Talib SIRdoctoranswerit_84161No ratings yet
- ThalcemiaDocument33 pagesThalcemiaRahul Kumar DiwakarNo ratings yet
- UntitledDocument3 pagesUntitledSandeep m rNo ratings yet
- Iron Deficiency AnemiaDocument12 pagesIron Deficiency AnemiaMargarita TorresNo ratings yet
- Math1 2019Document124 pagesMath1 2019David PattyNo ratings yet
- Eye & ENTDocument12 pagesEye & ENTShandar SadafNo ratings yet
- Mathematics: Teacher's ManualDocument178 pagesMathematics: Teacher's ManualAmali Gariga PeayaNo ratings yet
- Sample Oral Question2Document4 pagesSample Oral Question2Abouzr Mohammed ElsaidNo ratings yet
- Complications in Pediatric Otolaryngology PDFDocument635 pagesComplications in Pediatric Otolaryngology PDFwillyoueverlovemenkNo ratings yet
- Successful Management of Otitis Externa: Managing The DiseaseDocument5 pagesSuccessful Management of Otitis Externa: Managing The DiseaseAbouzr Mohammed ElsaidNo ratings yet
- Math1 2019Document124 pagesMath1 2019David PattyNo ratings yet
- Wa0010Document1 pageWa0010Abouzr Mohammed ElsaidNo ratings yet
- CME Quiz - Jan 2014 PDFDocument1 pageCME Quiz - Jan 2014 PDFAbouzr Mohammed ElsaidNo ratings yet
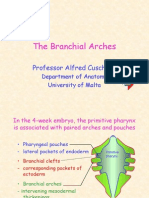
- The Branchial Arches: Professor Alfred CuschieriDocument13 pagesThe Branchial Arches: Professor Alfred CuschieriBabak BarghyNo ratings yet
- Nasopharyngeal Swab Procedure: BackgroundDocument1 pageNasopharyngeal Swab Procedure: BackgroundlalandNo ratings yet
- Dr. F. Lings Otolaryngology NotesDocument1,417 pagesDr. F. Lings Otolaryngology NotesAbouzr Mohammed Elsaid100% (3)
- Advances OCR FBDocument325 pagesAdvances OCR FBAbouzr Mohammed ElsaidNo ratings yet
- 2014 CPD Quiz July 2014Document1 page2014 CPD Quiz July 2014Abouzr Mohammed ElsaidNo ratings yet
- MCQS From April2008Document6 pagesMCQS From April2008Abouzr Mohammed ElsaidNo ratings yet
- Atls Summary ExaminationDocument14 pagesAtls Summary Examinationelnikety100% (2)
- MenuDocument8 pagesMenuAbouzr Mohammed ElsaidNo ratings yet
- Tumours of the Parapharyngeal SpaceDocument7 pagesTumours of the Parapharyngeal SpaceAbouzr Mohammed ElsaidNo ratings yet
- TonsillectomyDocument3 pagesTonsillectomyAbouzr Mohammed ElsaidNo ratings yet
- MCQ TrainingDocument3 pagesMCQ Trainingeldoc33100% (1)
- FINAL FRCA EXAM MCQS APRIL 2009Document16 pagesFINAL FRCA EXAM MCQS APRIL 2009Abouzr Mohammed ElsaidNo ratings yet
- Exam Additional Sample Questions AudDocument6 pagesExam Additional Sample Questions AudAbouzr Mohammed ElsaidNo ratings yet
- Ototoxic Effects From Gentamicin Ear DropsDocument2 pagesOtotoxic Effects From Gentamicin Ear DropsAbouzr Mohammed ElsaidNo ratings yet
- Imaging Safety InformationDocument20 pagesImaging Safety InformationAbouzr Mohammed ElsaidNo ratings yet
- What Percentage of Cleft LipDocument4 pagesWhat Percentage of Cleft LipAbouzr Mohammed ElsaidNo ratings yet
- Intravenous FluidsDocument37 pagesIntravenous FluidsStella UmehNo ratings yet
- Make A Short DNA ModelDocument5 pagesMake A Short DNA ModelShashank TiwariNo ratings yet
- Linkage: Harshraj Subhash Shinde KKW, Cabt, NashikDocument14 pagesLinkage: Harshraj Subhash Shinde KKW, Cabt, Nashiksivaram888No ratings yet
- BiotechnologyDocument6 pagesBiotechnologyHiral Jodavat100% (1)
- 5 Mapping in Prokaryotes PDFDocument34 pages5 Mapping in Prokaryotes PDFSabesan TNo ratings yet
- PCR - Polymerase Chain ReactionDocument37 pagesPCR - Polymerase Chain ReactionNandana Nayana Kumara100% (4)
- DNA ReplicationDocument70 pagesDNA ReplicationAnne Gabrielle Marapon AgsunodNo ratings yet
- NIPT-DNA TestDocument3 pagesNIPT-DNA Testfelicia susantoNo ratings yet
- Translation in ProkaryotesDocument7 pagesTranslation in ProkaryotesAkachukwu ObunikeNo ratings yet
- TTPB11ETHYLENE ShortDocument49 pagesTTPB11ETHYLENE ShortDiksha GahlotNo ratings yet
- Mutagenesis: Site-Specific: September 2005Document13 pagesMutagenesis: Site-Specific: September 2005Sarnam SinghNo ratings yet
- Biology Investigatory ProjectDocument20 pagesBiology Investigatory ProjectAnsia Meenaz100% (1)
- The Origin and Widespread Occurrence of Sli-BasedDocument17 pagesThe Origin and Widespread Occurrence of Sli-BasedDOWPLEX CREATIVENo ratings yet
- John Maynard Smith, Eörs Szathmáry - The Origins of Life - From The Birth of Life To The Origin of Language-Oxford University Press (2000)Document193 pagesJohn Maynard Smith, Eörs Szathmáry - The Origins of Life - From The Birth of Life To The Origin of Language-Oxford University Press (2000)MiraNo ratings yet
- The Central Dogma of Molecular BiologyDocument45 pagesThe Central Dogma of Molecular BiologyEirla Kneriz Trinidad67% (3)
- Ap - Cell Division - MeiosisDocument24 pagesAp - Cell Division - Meiosisapi-251015600No ratings yet
- MR Supple All 2014Document429 pagesMR Supple All 2014Regita Ayu LestariNo ratings yet
- Overview of Next Generation Sequencing TechnologiesDocument12 pagesOverview of Next Generation Sequencing TechnologiesiuventasNo ratings yet
- Week 3: Cell Modifications: General Biology 1Document3 pagesWeek 3: Cell Modifications: General Biology 1Florene Bhon GumapacNo ratings yet
- GIFT Selective Breeding Tilapia - MathewsDocument39 pagesGIFT Selective Breeding Tilapia - MathewsAlpesh JadhavNo ratings yet
- ViraPower Lentiviral Expression SystemsDocument52 pagesViraPower Lentiviral Expression Systemsxiaojun5244No ratings yet
- Download The Wiley Blackwell Handbook Of Childhood Social Development 3Rd Edition Peter K Smith all chapterDocument67 pagesDownload The Wiley Blackwell Handbook Of Childhood Social Development 3Rd Edition Peter K Smith all chapterveronica.reaver962100% (4)
- Data Mining MetaAnalysisDocument39 pagesData Mining MetaAnalysispaparountasNo ratings yet
- NASA Space Biology ProgramDocument52 pagesNASA Space Biology ProgramaksiiapNo ratings yet
- Learning-Activity-Worksheets - Science 9 - Q1-Week-3-4Document9 pagesLearning-Activity-Worksheets - Science 9 - Q1-Week-3-4GINALYNROSE ROSIQUENo ratings yet
- Virtual Lab-BuildingDNASEDocument5 pagesVirtual Lab-BuildingDNASEsmol ukeleleNo ratings yet
- Mystery of the Crooked Cell: Investigate Sickle Cell Anemia Using Gel ElectrophoresisDocument29 pagesMystery of the Crooked Cell: Investigate Sickle Cell Anemia Using Gel Electrophoresisschumon25No ratings yet
- Mitosis Worksheet & Diagram IdentificationDocument2 pagesMitosis Worksheet & Diagram IdentificationAli AshrafNo ratings yet