Professional Documents
Culture Documents
Hepatitis B Journal-Dikonversi
Uploaded by
rifahOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Hepatitis B Journal-Dikonversi
Uploaded by
rifahCopyright:
Available Formats
STATE OF THE ART REVIEW
Management of chronic hepatitis B
infection
Vinay Sundaram,1 Kris Kowdley2
1
Department of Medicine and
Comprehensive Transplant Center, ABSTRACT
Cedars-Sinai Medical Center, Los
Angeles, CA, USA
Hepatitis B virus (HBV) is a global health problem that can lead to cirrhosis and
2
Liver Care Network, Swedish hepatocellular carcinoma (HCC). Although HBV vaccination has reduced the prevalence Of
Medical Center, Seattle, WA 98104,
USA HBV infection, the burden of disease remains high. Treatment with antiviral drugs reduces
Correspondence to: K Kowdley the risk of liver disease and the development of HCC, and it can even reverse liver fibrosis.
Kris.Kowdley@swedish.org
Cite this as: BMJ 2015;351:h4263
However, challenges remain regarding optimal timing, as well as the modality and duration
doi: 10.1136/bmj.h4263 of treatment. Currently approved drugs include pegylated interferon and nucleos(t)ide
analogs. Nucleos(t)ide analogs are better tolerated and provide excellent viral suppression
with a low risk of antiviral resistance, but pegylated interferon offers the benefit of a finite
duration of treatment. Monitoring of hepatitis B surface antigen (HBsAg) levels may help
to predict the likelihood of response to treatment, particularly for pegylated interferon.
Prolonged treatment is usually needed with oral antiviral agents, and relapse is common if
treatment is discontinued. New treatments that result in sustained clearance of HBV DNA
and the clearance of HBsAg are needed.
Introduction treatment modalities to use, the effect of treatment on
Hepatitis B virus (HBV) is a major global health bur- the development of HBV related complications, and when
den—240 million patients are estimated to be chroni- to consider stopping treatment. Management in special
cally infected.1 2 About 30% of patients with chronic HBV populations infected with HBV, future treatments, and
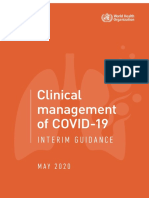
develop liver cirrhosis, and nearly 23% of these decom- the potential for viral eradication will also be reviewed.
pensate within five years.3 4 (fig 1) Research on the long
term efficacy of HBV treatment, the impact of treatment on Incidence and prevalence
the progression of liver disease and regression of cirrhosis, About 240 million people are infected with HBV world-
the utility of combination therapy, and strategies to man- wide and nearly 780000 people die from HBV related
age patients coinfected with HIV and hepatitis delta virus complications each year.5 Furthermore, nearly 50% of the
(HDV) is ongoing. This research will inform decisions about mortality secondary to hepatocellular carcinoma (HCC)
the optimal timing of treatment initiation, the appropri- in 2010 was associated with HBV.6 In the United States
ateness of treatment withdrawal, and the role of serologic alone nearly 704000 people have HBV infection.7
markers in predicting the response to treatment. A systematic review from 2012 estimated that nearly
This review will focus on the clinical management of 1.32 million people with HBV infection in the US were
chronic HBV infection. It will discuss the epidemiology foreign born, with 58% having emigrated from Asia. 8
and life cycle of the disease, the accuracy of non-invasive Regions of the world considered to have high prevalence
testing for fibrosis in HBV, when to start treatment, which (>7%) include China, South East Asia, Africa, the Pacific
Liver cancer CHCC3
4-6% of people with chronic
HBV infection develop HCC
Acute infection
›90% of infected children Cirrhosis
progress to chronic disease Chronic Infection 30% of people with chronic Liver transplantation Death
‹5% of infected adults HBV infection develop cirrhosis
progress to chronic disease
Liver failure Cdecompensation3
23% of patients decompensate
within 5 years of developing
cirrhosis
Fig 1| Natural course of hepatitis B virus (HBV) disease progression. HCC=hepatocellular carcinoma
For personal use only 1 of 12
STATE OF THE ART REVIEW
Serologic indicators of hepatitis B virus (HBV) infection The availability of the HBV vaccine since 1981 has led
Hepatitis B surface antigen (HBsAg): viral envelope surface protein, primary marker of HBV to a substantial decrease in the incidence of HBV infec-
infection tion and its sequelae such as HCC.11 Population studies
Hepatitis B surface antibody (anti-HBs): antibody that recognizes HBsAg; indicator of have shown that the proportion of children in Taiwan
immunity to HBV who are hepatitis B surface antigen (HBsAg) positive
Hepatitis B core antibody (anti-HBc): antibody that recognizes the intracellular core antigen decreased from 10% in 1984 to 0.9% in 2009, 12 while
Anti-HBc IgM: marker of acute infection (may also be raised in acute exacerbation of chronic in the US, the prevalence of HBV infection decreased in
HBV) people aged 6-19 years (from 1.9% to 0.6%; P<0.01) and
Anti-HBc IgG: marker of chronic infection 20-49 years of age (5.9% to 4.6%; P<0.01).13
Hepatitis B e antigen (HBeAg): secretory protein produced by translation of the precore
region of the HBV genome Sources and selection criteria
Hepatitis B e antibody (anti-HBe): antibody that recognizes HBeAg We used the terms “hepatitis B”, “hepatitis B treatment”,
“antiviral resistance”, “transient elastography”, “sur-
Islands, parts of the Middle East, and the Amazon basin.9 face antigen”, “hepatocellular carcinoma”, “nucleos(t)
Areas of intermediate prevalence (2-7%) include south ide analog”, “pregnancy”, “hepatitis delta”, “human
central and southwest Asia, eastern and southern Europe, immunodeficiency virus”, “chemotherapy”, and “future
Russia, Central America, and South America. Countries therapies” alone and in combination to search PubMed
of low prevalence (<2%) are primarily the US, western and Google Scholar from the year 2000 to 1 April 2015.
Europe, Australia, and Japan.2 Landmark studies before that date were also included. In
Because of the low likelihood of symptoms related to addition, we searched bibliographies of articles for rel-
chronic HBV infection, the true incidence is difficult to evant studies. Where relevant, we incorporated practice
determine. guidelines from the American Association for Study of
In areas of the world with a high prevalence of HBV, Liver Diseases (AASLD, 2009), European Association for
perinatal transmission is the main mode of spread, the Study of the Liver (EASL, 2012), and the Asian Pacific
whereas in countries with lower prevalence sexual expo- Association for Study of the Liver (APASL, 2012).10 14 15
sure is principally responsible for transmission.2 The We also reviewed abstracts from the 65th annual meeting
risk of infection is greater in those with a high number of the American Association for the Study of Liver Dis-
of sexual partners, homosexual males, and those with eases (Boston, November 2014), and the 49th annual
other sexually transmitted diseases.10 Blood borne trans- meeting of the European Association for the Study of the
mission of HBV may still occur in developing countries.2 Liver (London, April 2014). Evidence was obtained pri-
marily from randomized controlled trials.
HBeAg
Anti-HBe
Diagnosis and initial evaluation
The serologic indicators for HBV infection include HBsAg,
hepatitis B surface antibody (anti-HBs), hepatitis B e
antigen (HBeAg), hepatitis B e antibody (anti-HBe), and
HBV DNA
ALT
hepatitis B core antibody (IgM and IgG; (anti-HBc) ) (box).
HBeAg Serum HBsAg is the primary marker of infection. Once
Anti-HBe the diagnosis of HBV has been made on the basis of posi-
tive HBsAg, further evaluation should be performed by
measuring alanine aminotransferase (ALT), HBV DNA,
and anti-HBc IgG, as well as assessing HBeAg status and
liver fibrosis.10 14 15 Screening for coinfection with HIV
Immune tolerance Immune clearance Inactive carrier state
HBeAg+/-CHB
and hepatitis C virus is also recommended.14
LIVER HISTOLOGICAL ACTIVITY Phases of HBV infection
Mild Moderate/severe None/mild The natural course of chronic HBV infection can be
broadly classified into four stages: immune tolerance,
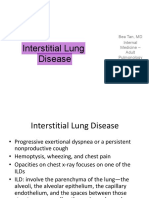
Fig 2| Phases of HBV infection. The immune tolerance phase occurs in patients who acquire HBV immune clearance, inactive carrier state, and reactivation
infection perinatally or in childhood and may last for 20-30 years. It is characterized by HBeAg
or HBeAg negative chronic hepatitis B. Figure 2 depicts
positivity, high HBV DNA levels (>20000 IU/mL), normal ALT values, and high HBsAg levels
>100000 IU/mL). During this phase, the virus is not cytopathic and minimal hepatic inflammation the immune tolerance, immune clearance, and inactive
occurs. In the immune clearance phase, the host immune system attempts to eliminate infected carrier phases.
hepatocytes through a T cell mediated immune response to viral antigens, leading to hepatocyte
apoptosis. Subsequently ALT levels rise above normal, HBV DNA levels fluctuate, and hepatic HBeAg negative chronic HBV
inflammation occurs. The immune response may ultimately lead to HBeAg seroconversion, After HBeAg seroconversion, a subset of patients may
defined as loss of HBeAg and development of anti-HBe. The inactive carrier state occurs after enter a disease state of viral reactivation, known as
the immune clearance phase and is characterized by the presence of HBsAg in serum, HBeAg HBeAg negative chronic HBV. Similar to the inactive car-
seroconversion, low levels of serum HBV DNA (<2000 IU/mL), and normal ALT concentrations. The
rier phase, this condition is also denoted by the absence
inactive carrier state may last indefinitely and potentially lead to loss of HBsAg. Abbreviations:
ALT=alanine aminotransferase; anti-HBe=hepatitis B e antigen antibody; CHB=chronic hepatitis of HBeAg. The main reason for HBeAg negativity is the
B infection; HBeAg=hepatitis B e antigen; HBsAg=hepatitis B surface antigen; HBV=hepatitis B presence of the precore stop codon mutation (G1896A),
virus Reproduced, with permission, from Yim and Lok16 which is selected during the immune clearance phase and
For personal use only 2 of 12
STATE OF THE ART REVIEW
becomes dominant, while the wild-type e antigen produc- formula: (age (years)×AST (U/L))/((platelets (109/L))×(ALT
ing virus is eliminated.17 Patients with HBeAg negative (U/L)1/2).33
disease have double the risk of progressing to cirrhosis A meta-analysis of 39 studies published in 2015 evalu-
than those with HBeAg positive infection.18 It is therefore ated the efficacy of APRI and FIB-4 in accurately assess-
crucial that the inactive carrier state is accurately differ- ing liver fibrosis in HBV. When the APRI threshold was
entiated from HBeAg negative HBV, because those with set at 0.5, sensitivity to predict advanced fibrosis was
HBeAg negative HBV will benefit from treatment. 73.0% and specificity was 54.5%; at a threshold of 1.0,
In addition, the double A1762T/G1764A mutation, sensitivity was 50.0% and specificity was 83.0%; and at
also known as the basal core promoter mutation, is a threshold of 1.5, sensitivity was 33.0% and specificity
associated with HBeAg negativity owing to decreased was 91.0%. With regard to FIB-4 for detecting advanced
production of the precore mRNA, which leads to reduced fibrosis, a threshold of below 1.45 and above 3.25 yielded
levels of HBeAg.19 20 People with HBeAg negative disease a sensitivity of 78.6% and a specificity of 98.0%.34 The
associated with the basal core promoter mutation are at meta-analysis concluded that these tests have moderate
increased risk of progression to cirrhosis21 and HCC,22 23 diagnostic accuracy for predicting fibrosis in chronic HBV
independent of HBV DNA level. infection.
Occult HBV infection Transient elastography
Occult HBV infection is defined as the presence of HBV Transient elastography uses ultrasound elastography
DNA in the liver and the absence of detectable HBsAg to assess the amount of liver stiffness as a surrogate of
using currently available assays, with or without the hepatic fibrosis.35 The outcome is measured in kPa and
presence of HBV DNA in the serum.24 HBV DNA levels ranges from 2.5 kPa to 75 kPa, with 5 kPa often desig-
are often less than 200 IU/mL. Occult HBV infection is nated as normal and 13.4 kPa or more as cirrhosis.36-38
more common in patients with hepatitis C virus (HCV) Several studies have investigated the utility of this
infection. In these patients it is associated with a greater test in determining the degree of liver fibrosis in patients
risk of progression to cirrhosis and development of HCC, with HBV. A study of 202 patients with HBV found that
as well as a shorter survival time.25 26 Patients with nega- this measure correlated well with stage of fibrosis on
tive HBsAg but with serum HBV DNA levels comparable liver biopsy (r=0.65).39 In a meta-analysis of 50 studies
to those found in overt HBV are classified as having false assessing the reliability of transient elastography for all
occult HBV infection as a result of infection with HBV causes of liver cirrhosis, the mean area under the receiver
escape mutants that are not recognized by commercial operating characteristic (AUROC) curve for the diagnosis
HBsAg assays.27 28 Such patients should be treated in the of cirrhosis was 0.94, with an optimal cut-off value of
same manner as those with overt HBV infection.28 13.01 kPa. This indicates that transient elastography is a
reliable technique for detecting cirrhosis regardless of the
Assessment of liver fibrosis cause.40 Another meta-analysis published in 2012 of 18
Because treatment is indicated for those with stage studies of patients with HBV, found that the mean AUROC
2 fibrosis or greater, it is often necessary to stage the curve was 0.93 for liver cirrhosis. A cut-off value of 11.7
degree of hepatic fibrosis. Furthermore, patients aged yielded a sensitivity and specificity for liver cirrhosis of
30 years or more can have stages 2-4 liver fibrosis even 84.6% and 81.5%, respectively.41
with persistently normal ALT concentrations.10 14 29 The
measurement of serum ALT may therefore not be a reli- Treatment initiation
able way to determine the extent of liver injury, and a The decision to begin treatment is based on the goals of
recent meta-analysis of nine studies showed that 27.8% treatment, including suppression of HBV DNA levels, nor-
of patients had stages 2-4 fibrosis even with normal ALT malization of ALT, and HBeAg seroconversion in HBeAg
concentrations.30 positive patients as well as patient characteristics, includ-
Although liver biopsy is considered the gold standard ing presence or absence of cirrhosis and hepatitis B inac-
for this indication there are concerns regarding sampling tive carrier state.
error—discordance in fibrosis stage occurs in up to 33% of
biopsies. In addition, complications such as hemorrhage People with cirrhosis
occur in up to 1/2500 biopsies, and pain occurs in up to In patients with cirrhosis, guidelines agree that those
84% of patients.31 Non-invasive evaluation of liver fibro- with decompensated cirrhosis should be treated with
sis can be considered as an alternative to biopsy. a nucleos(t)ide analogs, regardless of HBV DNA or ALT
level.10 14 15 However, the approach to the treatment of
Serologic biomarkers patients with compensated cirrhosis differs.
Among serologic biomarkers of liver fibrosis, the aspar- EASL recommendations state that treatment should
tate aminotransferase-to-platelet ratio index (APRI) and be considered in all patients with compensated cirrho-
fibrosis index based on the four factors (FIB-4) have been sis irrespective of ALT concentration or HBV viral load.14
most widely studied in patients with HBV. However, both AASLD and APASL recommendations
APRI is based on the ratio of aspartate aminotrans- suggest that patients with compensated cirrhosis and a
ferase (AST) concentration to platelet count.32 FIB-4 viral load 2000 IU/mL or more should be treated, whereas
was initially derived as a measure of fibrosis in a cohort monitoring of ALT and HBV DNA values can be consid-
of patients infected with both HCV and HIV using the ered for those with a viral load less than 2000 IU/mL.10 15
For personal use only 3 of 12
STATE OF THE ART REVIEW
Table 1 | Guideline recommendations on treatment initiation in patients with hepatitis B virus ALT concentration, HBV viral load, and HBeAg status
(HBV) infection are the most important. An ALT concentration of 30
Patient characteristics AASLD (2009) EASL (2012) APASL (2012) U/L in men and 19 U/L in women with HBV should be
HBeAg status considered the upper limit of normal. 46 Table 1 shows
Positive HBV DNA >20 000 IU/mL HBV DNA > 2000 IU/mL HBV DNA >20 000 IU/mL recommendations from the AASLD, EASL, and APASL
and ALT>2× upper limit of with ALT> upper limit of and ALT >2× upper limit of
normal normal or biopsy with normal
guidelines on when to start HBV therapy.
moderate fibrosis or
inflammation Predictors of treatment outcome
Negative HBV DNA >2000 IU/mL and HBV DNA >2000 IU/mL HBV DNA >2000 IU/mL and Evidence has consistently shown that the most important
ALT > upper limit of normal with ALT > upper limit of ALT> upper limit of normal
or stage 2 fibrosis normal or biopsy with or stage 2 fibrosis
outcome of treatment is suppression of HBV viral load
moderate fibrosis or because this parameter strongly correlates with the risk
inflammation of progression to cirrhosis and development of HCC.47
Cirrhosis In the Risk Evaluation of Viral Load Elevation and Asso-
Compensated HBV DNA >2000 IU/mL All patients regardless of HBV DNA >2000 IU/mL ciated Liver Disease/Cancer-HBV (REVEAL-HBV) cohort
decompensation or HBV
study, Cox regression adjusting for ALT concentration and
DNA level
Decompensated All patients All patients regardless of All patients HBeAg status showed that increasing HBV DNA level was
decompensation or HBV the strongest independent predictor of progression to cir-
DNA level rhosis.48 Additional data from this cohort showed that
AASLD=American Association for Study of Liver Diseases; ALT=alanine aminotransferase; APASL=Asian Pacific Association for
greater than 2000 IU/mL HBV DNA was the strongest risk
Study of the Liver; EASL=European Association for the Study of the Liver; HBeAg=hepatitis B e antigen.
factor for HCC, when controlling for HBeAg status, ALT
People without cirrhosis concentration, and cirrhosis. 49 Furthermore, patients
In people without cirrhosis, recommendations from whose HBV DNA dropped to less than 2000 IU/mL from
guidelines and from a panel of experts suggest that for baseline had a significantly lower risk of developing HCC
those in the immune tolerant phase, observation and (hazard ratio 2.25, 0.68 to 7.37 compared with controls)
monitoring of ALT and HBV DNA values every three to than those whose HBV DNA level persisted at 2000-
six months is appropriate, given the lack of data showing 20000 IU/mL (3.12, 1.09 to 8.89), 20000-200000 IU/
a benefit of treatment and the potential for antiviral resist- mL (8.85, 3.85 to 20.35), or greater than 200000 IU/mL
ance.10 14 15 42 In addition, a recent double blind rand- (16.78, 7.33 to 38.29).50
omized controlled trial of 126 immune tolerant patients,
as determined by HBeAg and normal ALT concentration, Currently available treatments
showed an HBeAg seroconversion rate of less than 5% Two therapeutic approaches are available for both HBeAg
after four years of nucleos(t)ide analog treatment.43 positive and HBeAg negative patients: finite therapy and
long term suppressive therapy. The goal of the first strat-
People in the inactive carrier state egy is sustained suppression of viral replication after the
The same guidelines also recommend that close moni- completion of treatment through the induction of the
toring rather than treatment is appropriate for people in inactive carrier state of HBV. This is designated by nor-
the inactive carrier state.10 14 15 Although patients in this mal ALT concentrations, HBV DNA less than 2000 IU/
phase usually have a low risk of disease progression, a mL, and, specifically for HBeAg positive patients, sero-
cohort study of 146 inactive carriers over a 23 years of conversion of HBeAg to anti-HBeAg. This strategy uses
follow-up found that 43 patients had increases in ALT treatment with pegylated interferon for 48 weeks. The
levels to above normal, one had spontaneous reactivation second approach aims to obtain rapid and long term viral
to the HBeAg negative state, and two developed HCC.44 In suppression with the use of oral nucleos(t)ide analogs,
a larger cohort of 20069 patients in the inactive carrier although the duration of treatment may be indefinite.
phase, the annual incidence rates of HCC and liver related
death were 0.06% and 0.04%, respectively, compared Pegylated interferon
with 0.02%, and 0.02% for controls. Furthermore, the The purpose of using pegylated interferon is to provide
hazard ratios were 4.6 (95% confidence interval 2.5 to the patient with a finite duration of treatment. Because
8.3) for the development of HCC and 2.1 (1.1 to 4.1) for pegylated interferon is associated with multiple toxici-
liver related mortality compared with controls.45 These ties, including fatigue, a flu-like reaction, anemia, pan-
findings emphasize the importance of continued surveil- cytopenia, and depression (in 20-30% of patients),51 it
lance of carriers with inactive disease for HCC. Further- is important to determine which patients will respond
more, given the potential for liver related complications to this drug before starting treatment. Characteristics
during the inactive carrier state even in people without indicating a favorable response include low HBV DNA
cirrhosis, treatment should be considered in all patients levels, high levels of ALT and HBV, presence of the HBV
with cirrhosis, regardless of HBV DNA level. genotype A or B, and lack of advanced liver disease.52 53
The IL28B polymorphism may also predict response
Other patients to interferon based therapy because studies have indi-
In the remainder of patients the decision to start therapy cated greater decreases in HBV DNA and higher rates
should be based on a variety of factors including HBeAg of HBeAg to anti-HBe seroconversion or HBsAg loss in
status, ALT concentration, HBV viral load, age (<40 v >40 those who have the CC genotype rather than the CT or
years), and stage of liver fibrosis. Among these variables, TT polymorphism.54
For personal use only 4 of 12
STATE OF THE ART REVIEW
In one of the largest trials to evaluate the efficacy of international guidelines recommend only entecavir and
pegylated interferon in HBV, 814 HBeAg positive patients tenofovir as first line therapy for nucleos(t)ide analog
were given pegylated interferon, lamivudine, or a com- naive patients with HBV.10 14 15 Both of these drugs are
bination of both for 48 weeks and followed up for 24 well tolerated overall with minimal adverse effects.
weeks after treatment was discontinued. Compared with
patients assigned to lamivudine alone, the HBeAg to anti- Entecavir
HBeAg seroconversion rate was significantly greater in Registration trials that compared lamivudine with ente-
those taking pegylated interferon monotherapy (32% cavir in HBeAg positive and HBeAg negative treatment
v 19%; P<0.001) or combination therapy (27% v 19%; naive patients showed that entecavir had significantly
P=0.02).55 In addition, 16 patients given interferon sero- greater efficacy in reducing HBV DNA to undetectable
converted from HBsAg to anti-HBsAg, compared with levels and normalizing ALT over 48 weeks.60 61 A rand-
none who received lamivudine (P=0.001). In a retrospec- omized controlled trial of 715 HBeAg positive patients
tive analysis of 808 patients, HBeAg positive patients with showed that entecavir significantly increased the pro-
HBV genotype A, high ALT concentration, and low HBV portion of patients with undetectable HBV DNA (67% v
DNA level had a 54% predicted probability of a sustained 36%; P<0.001) and normalization of ALT (68% v 60%;
response to pegylated interferon, defined as HBeAg sero- P=0.02).60 Reported rates of adverse events were 86% in
conversion and HBV DNA level less than 2000 IU/mL52 the entecavir arm and 84% in the lamivudine arm (not
Because interferon seems to be successful in only a significant). Common adverse events included diarrhea,
third of patients, studies have assessed how to improve fatigue, abdominal pain, and cough.
the efficacy of interferon based therapy, including com- A separate randomized controlled trial of 648 HBeAg
bination therapy with nucleos(t)ide analogs. However, negative patients randomized to entecavir or lamivudine
regimens involving interferon combined with nucleos(t) found that entecavir significantly increased the propor-
ide analogs or ribavirin did not improve the response tion of patients with undetectable HBV DNA levels (90%
in HBeAg positive and HBeAg negative patients with v 72%; P<0.001) and ALT normalization (78% v 71%;
HBV.55-57 P=0.045).61 Rates of adverse events, including fatigue,
Regarding the duration of treatment, the NEPTUNE headache, diarrhea, and nausea, were similar between
randomized trial showed that among 544 patients with the two study groups—76% in people taking entecavir
HBeAg positive HBV, the highest response was associ- and 79% in those taking lamivudine. However, 6% of
ated with pegylated interferon at a dosage of 180 μg once those taking entecavir and 9% of those taking lamivudine
weekly for 48 weeks (36.2% HBeAg seroconversion rate) discontinued treatment.
rather than 180 μg or 90 μg for 24 weeks (25.8% and These findings were confirmed in a randomized con-
14.1%, respectively; P values not provided). 58 Another trolled trial that compared lamivudine with entecavir in
randomized controlled trial of 128 HBeAg negative 709 HBeAg positive patients over 96 weeks. This trial
patients, 94% of whom had HBV genotype D, compared demonstrated superiority of entecavir in the reduction
48 weeks of pegylated interferon (180 µg/week; n=51); of HBV DNA (80% v 39%; P<0.001) and normalization of
96 weeks of pegylated interferon (48 weeks at 180 μg/ ALT (87% v 79%; P=0.005), although cumulative HBeAg
week then 48 weeks at 135 μg/week; n=52); and 48 seroconversion was similar between the two groups.62 No
weeks of pegylated interferon (180 μg/week) plus lamivu- patients taking entecavir developed resistance during the
dine (100 mg/day) then 48 weeks of pegylated interferon study period.
alone (135 μg/week) (n=25). It found that 48 weeks after Regarding HBeAg negative patients, a randomized
finishing treatment, HBV DNA was less than 2000 IU/ controlled trial of 648 patients showed that entecavir
mL in significantly more patients who were treated for significantly increased the proportion of patients with
96 weeks with pegylated interferon alone than in those undetectable HBV DNA compared with lamivudine (90%
treated for 48 weeks with pegylated interferon mono- v 72%; P<0.001) and with normalization of ALT (78% v
therapy (28.8% v 11.8%; P=0.03). The rate of normali- 71%; P=0.045).61 Follow-up of this cohort for five years
zation of ALT was also higher in the group receiving 96 detected entecavir resistance in one patient, HBeAg
weeks of pegylated interferon monotherapy, but this was seroconversion in 23% of patients, and loss of HBsAg in
not significant (25% v 11.8%; P=0.08).59 Furthermore, 1.4%.63
the addition of lamivudine during the first 48 weeks of An observational study reported a 1.2% cumulative
treatment did not lead to significantly higher rates of sus- probability of entecavir resistance in treatment naive
tained HBV DNA suppression to less than 2000 IU/mL at patients, whereas patients refractory to lamivudine had a
48 weeks after stopping treatment (28.8% for monother- lower barrier to developing resistance mutations, leading
apy v 20% for combination treatment). Adverse effects to a 51% cumulative probability of developing resistance
associated with pegylated interferon were seen in 20-30% mutations over five years.64 These findings were similar to
of patients, but data on the rate of individual side effects a more recent prospective study that reported a cumula-
were seldom reported in the above trials. tive 1.2% incidence of entecavir resistance in HBeAg posi-
tive, treatment naive patients over three years’ duration.65
Nucleos(t)ide analogs Regarding the safety profile of entecavir, one retrospec-
Several nucleos(t)ide analogs are available for the treat- tive study identified five cases of lactic acidosis among
ment of HBV including lamivudine, adefovir, telbivudine, 16 entecavir treated patients with decompensated liver
entecavir, and tenofovir disoproxil fumarate. However, disease, all of whom had MELD (model for end stage liver
For personal use only 5 of 12
STATE OF THE ART REVIEW
Table 2 | Guideline recommendations for management of antiviral resistance in patients with developed adefovir resistance mutations. 74 Although
hepatitis B virus infection resistance to entecavir is rare, treatment of this condition
Drug AASLD (2009) EASL (2012) with tenofovir monotherapy is comparable to tenofovir
Lamivudine Add adefovir or tenofovir Switch to tenofovir or add adefovir if tenofovir not available and entecavir combination therapy, with 71% and 73%
Telbivudine Add adefovir or tenofovir; Switch to or add tenofovir of patients obtaining an undetectable HBV DNA level at
switch to emtricitabine
48 weeks.75
Adefovir Add lamivudine; switch to or Switch to entecavir or tenofovir if naive to lamivudine; switch to
add entecavir; switch to or tenofovir and add nucleoside analogue if has been exposed to
add tenofovir lamivudine Monitoring surface antigen level
Entecavir Switch to tenofovir or Switch to or add tenofovir HBsAg has traditionally been used to diagnose HBV infec-
tenofovir + emtricitabine tion and two commercially available assays for measuring
AASLD=American Association for Study of Liver Diseases;EASL=EuropeanAssociation for the Study of the Liver.
HBsAg—the Architect HBsAg assay (Abbott Diagnostics)76
and the Elecsys HBsAg II quant assay (Roche Diagnos-
disease) scores of 22 or greater.66 In two subsequent stud- tics)77—have recently been developed. Recent studies
ies of patients with decompensated cirrhosis, no cases of suggest that the measurement of HBsAg titers may also
lactic acidosis were reported. 67 68 be useful for predicting the course of HBV infection and
assessing treatment response.78
Tenofovir disoproxil fumarate Several studies have demonstrated the utility of meas-
Initial randomized controlled trial data comparing teno- uring HBsAg to establish the patient’s clinical course. In
fovir with adefovir in 846 HBeAg positive and 603 HBeAg HBeAg positive patients in the immune tolerant phase, a
negative patients showed that tenofovir significantly HBsAg value of greater than 25 000 IU/mL yielded a 90%
increased normalization of ALT (68% v 54%; P=0.03) positive predictive value for mild liver fibrosis.79 Another
and loss of HBsAg (3% v 0%; P=0.02) without evidence study showed that in HBeAg positive patients, HBsAg lev-
of resistance to tenofovir.69 After eight years of follow-up els of 38 500 IU/mL or less were associated with moderate
of this patient cohort, no resistance mutations have been to severe fibrosis.80
detected in HBeAg positive or HBeAg negative patients HBsAg levels may also help distinguish between inac-
receiving long term tenofovir, with most cases of virologic tive carriers and chronic active HBeAg negative infection.
breakthrough being caused by non-adherence.70 Several studies showed that inactive carriers have lower
Studies of combination therapy with two nucleos(t) HBsAg levels, with HBsAg less than 1000 U/mL having a
ide analogs have found marginal benefit over mono- 87.9% positive predictive value and 96.7% negative pre-
therapy overall. One randomized trial of 379 treatment dictive value for the patient having HBV DNA less than
naive patients compared entecavir monotherapy with 2000 IU/mL.81 The REVEAL-HBV study group showed
combined entecavir and tenofovir in naive HBeAg posi- that HBsAg less than 1000 IU/mL is associated with a
tive and negative patients. It found that entecavir was lower risk of developing HCC.47
as effective as combination therapy, although patients With regard to HBsAg and treatment response, data
with HBV DNA levels greater than 108 IU/mL had a sig- suggest that lower pretreatment HBsAg values are asso-
nificantly greater likelihood of having undetectable DNA ciated with a greater response to pegylated interferon,
levels at 100 weeks.71 Additional studies have shown that and that HBsAg titers may be used as an on-treatment
tenofovir monotherapy has comparable efficacy to tenofo- marker for sustained treatment response to this drug.82 A
vir combined with emtricitabine (Truvada) in both naive reduction in HBsAg to 300 IU/mL or less after six months
and lamivudine experienced patients. 43 72 of treatment correlates with a sustained response at 12
months after completion of therapy, defined as anti-HBe
Antiviral resistance seroconversion and HBV DNA less than 2000 IU/mL.83
Treatment of antiviral resistance involves selection Furthermore, patients who do not have a reduction in
of an agent without cross resistance to the mutation, HBsAg levels at week 12 of pegylated interferon treat-
thereby reducing the risk of selecting viral strains with ment have a low likelihood of sustained response or
mutations that lead to multidrug resistance. This is best HBsAg loss.84
accomplished by switching to a drug with a high barrier One study of 48 HBeAg negative patients treated with
to resistance instead of adding extra drug (table 2).14 15 pegylated interferon for 48 weeks found that people
Switching to tenofovir is appropriate in patients with whose HBsAg dropped by greater than 0.5 log IU/mL at
lamivudine resistance. In a study of 131 patients in whom week 12 and greater than 1 log IU/mL at week 24 had an
treatment with lamivudine or adefovir alone, sequen- 89% and 92% positive predictive value, respectively, of
tially, or in combination was ineffective, tenofovir was an having a sustained response after completing treatment.
effective rescue therapy and nearly 80% of patients given By contrast, patients in whom HBsAg did not drop had
tenofovir monotherapy achieved an undetectable HBV only a 10% chance of response, defined as undetectable
DNA level.73 Resistance was shown in 62% of patients HBV DNA at 24 weeks after treatment stopped.85
taking lamivudine and 19% taking adefovir.73 Entecavir
has also been shown to be effective in people who are Treatment withdrawal
resistant to adefovir. One cohort study of 161 patients, of Evidence from a randomized controlled trial of 548
whom 34% had been previously treated with nucleos(t) patients supports the notion that pegylated interferon
ide analogs, found that treatment with adefovir did not should be stopped in any of the following scenarios:
reduce the efficacy of entecavir even in those who had absence of a decline in HBV DNA level to 20000 IU/mL
For personal use only 6 of 12
STATE OF THE ART REVIEW
or less, lack of a reduction of HBsAg to less than 1500 U/ a landmark study in patients with advanced fibrosis
mL at week 12 or 24, 58 and completion of 48 weeks of from East Asia and the Pacific showed that a response to
treatment.10 lamivudine delays progression of HBV related liver dis-
Withdrawal of nucleos(t)ide analogs can be considered ease in terms of hepatic decompensation, liver related
six to 12 months after anti-HBe seroconversion in patients mortality, and development of HCC.92 The study rand-
who are HBeAg positive before they start treatment, and omized 651 patients to receive lamivudine or placebo;
after HBsAg loss in those who are HBeAg negative at the 7.8% of patients receiving lamivudine versus 17.7% of
start of treatment. 10 14 15 However, published findings those receiving placebo reached an end point of disease
suggest that relapse rates may be high after withdrawal progression (hazard ratio 0.45; P=0.001), and 3.9%
of treatment. of patients receiving lamivudine versus 7.4% of those
receiving placebo developed HCC (P=0.047).92
HBeAg positive patients Evidence on the effectiveness of entecavir and tenofovir
A single center prospective cohort study of 132 HBeAg in preventing complications of HBV has come primarily
positive patients showed that HBeAg seroconversion from observational studies. In a Japanese observational
occurred in 46 patients (35%) receiving nucleos(t)ide study, the cumulative five year incidence of HCC was sig-
analogs after a median duration of 26 months of treat- nificantly lower in 472 patients treated with entecavir
ment. Of nine patients who discontinued treatment after than in 1143 treatment naive patients (adjusted hazard
seroconversion and six months of consolidation therapy, ratio 0.37; P=0.03).93
only two had a sustained treatment response.86 Another retrospective-prospective cohort study that
In another retrospective study of 178 Korean patients compared 1446 entecavir treated patients with 424
with HBeAg positive HBV treated with lamivudine mono- untreated historical controls found no difference in
therapy who had attained a complete response (undetect- hepatic events in patients without cirrhosis. However,
able HBV DNA level, normalization of ALT, and loss of entecavir reduced liver related mortality (hazard ratio
HBeAg), the cumulative rate of relapse within five years 0.51, 0.34 to 0.78; P=0.002), occurrence of HCC (0.55,
of stopping treatment was 30.2%. Relapse occurred in 33 0.31 to 0.99; P=0.049), and liver related mortality (0.26,
of the 40 patients within the first two years.87 0.13 to 0.55; P<0.001) in patients with cirrhosis as deter-
mined by Cox proportional hazard regression.94
HBeAg negative patients In a Taiwanese national cohort study of more than
Studies on treatment withdrawal in HBeAg negative 21000 patients, treatment with nucleos(t)ide analogs
patients have typically been conducted in small samples. In was associated with a significantly lower seven year inci-
an observational cohort study of 33 Greek patients treated dence of HCC.95 Notably, however, most studies showing
for four or five years with adefovir, six years after stopping that nucleos(t)ide analogs reduce the risk of HCC have
treatment, 18 patients had an HBV DNA value less than been performed in Asian people, and studies that look
2000 IU/mL and 13 of them achieved HBsAg loss.88 at the effects of nucleos(t)ide analog treatment on risk of
A larger study evaluated relapse rates after withdrawal HCC are also needed in white people.96
of entecavir in 184 HBeAg negative patients with an
undetectable HBV DNA level for more than two years. It HIV coinfection
reported high relapse rates of 74.1% and 91.4% at 24 Among the estimated 40 million people infected with HIV
and 48 weeks, respectively, after stopping treatment. 89 worldwide, two to four million are chronically infected
In a randomized controlled study of vaccine therapy with HBV. HIV infection worsens the natural course of
in patients with HBV and undetectable HBV DNA after HBV infection by impairing the innate and adaptive
a median of three years of treatment with nucleos(t)ide immune responses to the virus. 97 98 This may lead to
analogs, discontinuation of treatment was associated increased rates of chronic HBV after acute infection and
with HBV reactivation in 97%, indicating that vaccination lower rates of HBeAg seroconversion or HBsAg loss with
does not reduce the risk of relapse after discontinuation of treatment.99 100
nucleos(t)ide analogs.90 Given the relatively high rate of In the Multicenter Cohort Study of 5293 homosexual
relapse after withdrawal of nucleos(t)ide analogs, treat- men, liver related mortality was higher in coinfected
ment discontinuation should be undertaken cautiously, patients than in those with HIV or HBV monoinfec-
particularly in HBeAg negative patients. tion, especially when CD4 cell nadir counts were low.101
The Euro-SIDA cohort also showed greater liver related
Outcomes of HBV treatment mortality in coinfected patients, with mortality increas-
Long term treatment with third generation nucleos(t) ing from 8% in HBV negative to 18% in HBV positive
ide analogs may lead to improvement in liver fibrosis people.102
and potentially reversal of cirrhosis. A five year study of When both HIV and HBV infections need to be treated,
entecavir treated patients documented the histological antiretroviral therapy using the combination of teno-
reversal of cirrhosis in four of 10 cases.63 Another study fovir and emtricitabine or lamivudine is preferred. 14 15
found that, among 96 patients with cirrhosis, 71 patients A retrospective study of 65 HBV and HIV coinfected
had regression of cirrhosis after five years of treatment patients showed that tenofovir was effective in patients
with tenofovir and successful viral suppression.91 with wild-type and lamivudine resistant HBV infection,
With regard to the effect of HBV treatment on the indicating that tenofovir can be used as a component
progression of liver disease and development of HCC, of HIV therapy even in those exposed to lamivudine.103
For personal use only 7 of 12
STATE OF THE ART REVIEW
and HDV are acquired simultaneously, or as a superin-
fection, whereby HDV infection occurs in a patient with
HBV infection.
Interferon based therapy is the primary treatment for
HDV. The Hep-Net International Delta Hepatitis Interven-
tion Study (HIDIT) group published a randomized trial
Viral entry Budding vescular that compared pegylated interferon alone (n=29), ade-
transport fovir alone (n=30), or combination therapy (n=31) for
treating HDV. It found that pegylated interferon, with or
without adefovir, led to sustained HDV clearance in 28%
Uncoating
Viral of patients 24 weeks after treatment. 106 However, long
assembly at term follow-up of this patient cohort found that more than
Recycling
endoplasmic
reticulum half of those with a sustained response 24 weeks after
the end of treatment relapsed, as defined by HDV ribo-
nucleic acid positive testing.107 The randomized double
Nuclear
compartment blind trial HIDIT-2 study evaluated prolonged treatment
Nuclear import
(-) strand synthesis with pegylated interferon, with (n=59) or without teno-
Removal of pgRNA fovir (n=61), for 96 weeks. Both treatments had similar
(+) strand synthesis efficacy with regard to sustained response 24 weeks after
treatment (23-30%), and the presence of cirrhosis was
associated with a higher response rate on multivariate
Integration of viral DNA analysis.108
into the host genome
Repair 3.5 kb pgRNA Pregnancy
In women of childbearing age, treatment aims to reduce
2.4/2.1 kb mRNA Encapsidation HBV transmission to the infant because the risk of devel-
pgRNA, HBcAG oping chronic HBV infection is high in those exposed
0.7 kb mRNA polyprotein
Transcription during birth. 109 Active-passive immunoprophylaxis
reduces mother to child transmission rates by 95%. 110
cccDNA Translation of
viral proteins The standard regimen involves administration of hepati-
tis B immune globulin and hepatitis B vaccination to the
infant. However, transmission may still occur even with
Cytoplasm
immunoprophylaxis in mothers who have an HBV DNA
level greater than 107 IU/mL.111
Fig 3 | Life cycle of hepatitis B virus (HBV). After infecting the hepatocyte, the HBV In women who are pregnant or planning pregnancy
genome is delivered into the nucleus where cellular enzymes repair the viral genome into in the near future, nucleos(t)ide analogs should be
covalently closed circular DNA (cccDNA). cccDNA acts as a template for transcription of used with caution because of the risk of mitochondrial
pregenomic and pre-core mRNA. The pregenomic RNA (pgRNA) is encapsulated by the
toxicity.10 However, in women with advanced fibrosis or
core particle and reverse transcribed by viral polymerase to form a single strand DNA
molecule. Subsequently, the pre-genome is degraded and the negative strand DNA acts as cirrhosis it has been suggested that treatment should be
a template for synthesis of a positive strand DNA molecule. The HBV genome is then either initiated and continued throughout pregnancy.109
encapsulated by the envelope to produce virions that are secreted out of the hepatocyte or A population based study that compared 339 women
recycled back to the nucleus as cccDNA, resulting in the formation of a steady state of 5-50 with cirrhosis with 6625 age matched controls found that
copies of cccDNA molecules per infected hepatocyte. Abbreviations: HBcAg=hepatitis B core those with underlying cirrhosis have the highest risk of
antigen. Reproduced, with permission, from Jayalakshmi and colleagues128 HBV associated decompensation in pregnancy, with an
associated mortality risk of 1.8% for mothers and 5.2%
A meta-analysis of 23 studies also demonstrated the for the fetus.112
efficacy of tenofovir in the suppression of HBV viremia, Women without advanced fibrosis and with HBV DNA
with no impact of previous lamivudine exposure or levels greater than 107 IU/mL can be considered for treat-
combination with emtricitabine. 104 Although evidence ment in the third trimester to prevent fetal transmission.
from this study suggests that tenofovir may have simi- Interferon should be avoided because animal studies
lar efficacy to combined tenofovir and emtricitabine, suggest that it may lead to fetal abortion and data from
combination therapy is still the preferred treatment for humans are not available.113 If nucleos(t)ide analogs are
coinfected patients.14 used, telbivudine and tenofovir are pregnancy category
B drugs. It has been shown that administration of either
Hepatitis delta of these drugs to highly viremic mothers leads to 0% HBV
HDV is a human RNA virus that encodes the delta anti- transmission to the fetus, compared with about 8% trans-
gen, which is subsequently encased in an envelope within mission in controls.114-116
HBsAg.105 Although HDV infection suppresses HBV rep- If antiviral therapy is started during pregnancy it
lication, it can lead to severe liver disease including ful- should be discontinued postpartum in mothers who
minant liver failure, end stage liver disease, and HCC. intend to breast feed. Even though these drugs are
HDV infection occurs as a coinfection, when both HBV secreted at low levels in breast milk, studies on the long
For personal use only 8 of 12
STATE OF THE ART REVIEW
Table 3 | Emerging treatments for hepatitis B virus (HBV) infection
Treatment Mechanism of action Phase Comments
131 132
Myrcludex-B Viral entry inhibitor Ia Targets sodium taurocholate cotransporting polypeptide, a receptor for HBV entry
Bay 41-4109
133
Viral nucleocapsid inhibitor I Part of the heteroaryldihydropyrimidine family, which decreases stability of the viral capsid by
misdirecting its assembly
134
GLS 4 Viral nucleocapsid inhibitor I Heteroaryldihydropyrimidine family
REP 9 AC
135
HBsAg release inhibitor Ib Blockssecretionof non-infectioussubviralparticlesthatmayact as decoys to immune system;in
combination with immune therapy may lead to HBsAg clearance
136
GS-9620 Toll-like receptor 7 agonist I Activation of toll-like receptor-7 induces innate immunity to inhibit HBV replication
137
DV-601 Therapeutic vaccine Ib Stimulates T cell and B cell antibody response against HBsAg; comprises HBsAg and HBcAg
138
Zinc finger proteins Block transcription of cccDNA Preclinical
Disubstituted sulfonamides (CCC-0975 and Reduce cccDNA levels Preclinical Inhibit cccDNA production
CCC-0346)139
cccDNA=covalently closed circular DNA; HBcAg=hepatitis B core antigen; HBsAg=hepatitis B surface antigen.
term safety in infants who were breast fed by mothers HBsAg negative, anti-HBc positive patients
taking HBV antiviral drugs are lacking. 117 Patients who are HBsAg negative but anti-HBc posi-
tive can also be considered for prophylactic nucleos(t)
HBV reactivation after immunosuppression ide analog therapy, even though reactivation (reverse
Patients infected with HBV who receive immunosuppres- seroconversion) rates are lower than in HBsAg positive
sive therapy are at risk of viral reactivation. Such patients patients, ranging from 5% in patients receiving biologic
include those who undergo bone marrow, stem cell, or agents to 20% in those receiving immunosuppression for
solid organ transplantation and those receiving chemo- stem cell transplantation.
therapy, anti-CD20 antibodies, or biologic agents (tumor In a randomized trial of 80 HBsAg negative and anti-
necrosis factor α inhibitors).118-120 Rates of HBV reactiva- HBc positive patients receiving chemotherapy, the rate of
tion range from 38% in those receiving tumor necrosis HBV reactivation was significantly lower in those receiv-
factor α inhibitors to as high as 80% in those undergoing ing entecavir prophylactically (n=41) than in those on
stem cell or solid organ transplantation and those receiv- pre-emptive treatment (n=39) (2% v 18%; P<0.05).126
ing anti-CD20 antibodies.121 Presentation varies from a However, a prospective cohort study evaluating pre-
mild increase in aminotransferase to fulminant liver emptive entecavir for HBV flares in 150 anti-HBc positive
failure.118 Because HBV reactivation is preventable with patients found that after rituximab based chemotherapy,
appropriate screening and treatment, testing all patients the incidence of HBV reactivation and HBV related hepa-
for HBsAg and anti-HBc, followed by an HBV DNA level titis flares was 10.4 and 6.4 per 100 person year and that
if positive, is recommended before immunosuppressive only four patients had a severe HBV flare without prophy-
therapy is started.122 lactic entecavir treatment.127 Currently, studies evaluating
the cost effectiveness of prophylactic versus pre-emptive
HBsAg positive patients nucleos(t)ide analog therapy in anti-HBc positive patients
Two randomized controlled trials have compared the are lacking.
efficacy of prophylactic versus pre-emptive antiviral
therapy in preventing HBV reactivation. In the first study, Emerging treatments
30 HBsAg positive patients undergoing chemotherapy Despite improvements in the treatment of chronic HBV
received lamivudine prophylactically or pre-emptively— infection, treatment is currently directed towards inhi-
that is, when a 10-fold increase in HBV DNA occurred bition of viral replication rather than complete elimina-
or HBV DNA was present in those who had undetectable tion of HBV. Future treatments that aim to inhibit various
HBV DNA at baseline. HBV reactivation occurred in 53% aspects of the HBV life cycle are in development (fig 3).
of the patients receiving pre-emptive lamivudine but none There are several potential therapeutic targets in the
of those receiving prophylactic lamivudine (P=0.002).123 HBV life cycle, including inhibition of viral entry into the
The second study of 51 HBsAg positive patients also hepatocyte, disruption of the viral nucleocapsid, degen-
showed that fewer patients receiving prophylactic lami- eration of covalently closed circular DNA, prevention of
vudine had HBV reactivation (12% v 56%; P=0.001).124 HBsAg release, and immune based therapies including
Because more than 50% of HBsAg positive patients have toll-like receptor agonists and therapeutic vaccines (table
viral reactivation in this setting, we suggest that all HBsAg 3).129 130
positive patients should receive nucleos(t)ide analogs
before immunosuppression and then for 12 weeks after Conclusion
discontinuation of immunosuppressive therapy, regard- HBV infection represents a global health burden that
less of DNA level.14 is associated with serious morbidity and mortality
Lamivudine is an appropriate and cost effective drug if untreated. Treatment strategies include pegylated
in this setting, particularly if treatment is expected to interferon for a finite duration or long term suppressive
be of finite duration.125 However, entecavir or tenofovir therapy with nucleos(t)ide analogs. Pegylated inter-
is recommended in those in whom treatment might be feron therapy has lower rates of sustained response
for an indefinite period, and entecavir may be preferable after treatment is stopped, and combination therapy
because of reduced renal toxicity.119 with nucleos(t)ide analogs does not improve efficacy.
For personal use only 9 of 12
STATE OF THE ART REVIEW
1 Goldstein ST, Zhou F, Hadler SC, et al. A mathematical model to estimate
RESEARCH QUESTIONS global hepatitis B disease burden and vaccination impact. Int J Epidemiol
Can serologic markers be developed to predict which 2005;34:1329-39.
2 Trepo C, Chan HL, Lok A. Hepatitis B virus infection. Lancet
patients have a low risk of relapse after withdrawal of
2014;384:2053-63.
nucleos(t)ide analogs? 3 Fattovich G, Giustina G, Schalm SW, et al. Occurrence of hepatocellular
Is finite therapy possible for hepatitis B e antigen negative carcinoma and decompensation in western European patients with
cirrhosis type B. The EUROHEP Study Group on Hepatitis B Virus and
infection?
Cirrhosis. Hepatology 1995;21:77-82.
Is prophylactic therapy with nucleos(t)ide analogs cost 4 Moyer LA, Mast EE. Hepatitis B: virology, epidemiology, disease, and
effective in patients with antibodies to the hepatitis B core prevention, and an overview of viral hepatitis. Am J Prevent Med
1994;10(suppl):45-55.
who are receiving immunosuppression?
5 WHO. Hepatitis B. Fact sheet 204. 2015. www.who.int/mediacentre/
Will treatment be developed to degrade covalently closed factsheets/fs204/en.
circular DNA and will this lead to a cure for hepatitis B virus 6 Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality
infection? from 235 causes of death for 20 age groups in 1990 and 2010: a
systematic analysis for the Global Burden of Disease Study 2010. Lancet
2012;380:2095-128.
7 Ioannou GN. Hepatitis B virus in the United States: infection, exposure,
ABBREVIATIONS and immunity rates in a nationally representative survey. Ann Intern Med
2011;154:319-28.
AASLD: American Association for Study of Liver Diseases 8 Kowdley KV, Wang CC, Welch S, et al. Prevalence of chronic hepatitis B
ALT: Alanine aminotransferase among foreign-born persons living in the United States by country of
origin. Hepatology 2012;56:422-33.
Anti-HBc: Hepatitis B core antibody 9 Te HS, Jensen DM. Epidemiology of hepatitis B and C viruses: a global
Anti-HBe: Hepatitis B e antibody overview. Clin Liver Dis 2010;14:1-21, vii.
10 Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology
Anti-HBs: Hepatitis B surface antibody 2009;50:661-2.
APASL: Asian Pacific Association for Study of the Liver 11 Chang MH, You SL, Chen CJ, et al. Decreased incidence of hepatocellular
carcinoma in hepatitis B vaccinees: a 20-year follow-up study. J Natl
AST: Aspartate aminotransferase
Cancer Inst 2009;101:1348-55.
APRI: Aspartate aminotransferase to platelet ratio index 12 Ni YH, Chang MH, Wu JF, et al. Minimization of hepatitis B infection by a
25-year universal vaccination program. J Hepatol 2012;57:730-5.
AUROC: Area under receiver operating characteristic
13 Wasley A, Kruszon-Moran D, Kuhnert W, et al. The prevalence of hepatitis
EASL: European Association for the Study of the Liver B virus infection in the United States in the era of vaccination. J Infect Dis
FIB-4: Fibrosis index based on the four factors 2010;202:192-201.
14 European Association for the Study of the Liver. EASL clinical practice
HBeAg: Hepatitis B e antigen guidelines: management of chronic hepatitis B virus infection. J Hepatol
HBsAg: Hepatitis B surface antigen 2012;57:167-85.
15 Liaw YF, Leung N, Kao JH, et al. Asian-Pacific consensus statement on
HBV: Hepatitis B virus the management of chronic hepatitis B: a 2012 update. Hepatol Int
HCC: Hepatocellular carcinoma 2012;6:531-61.
16 Yim HY, Lok AS-F. Natural history of chronic hepatitis B virus infection:
HCV: Hepatitis C virus what we knew in 1981 and what we know in 2005. Hepatology
HDV: Hepatitis delta virus 2006;43(suppl 1):S173-81.
17 Hadziyannis SJ, Vassilopoulos D. Hepatitis B e antigen-negative chronic
REVEAL-HBV: Risk Evaluation of Viral Load Elevation and hepatitis B. Hepatology 2001;34:617-24.
Associated Liver Disease/Cancer-HBV 18 Fattovich G, Bortolotti F, Donato F. Natural history of chronic hepatitis
B: special emphasis on disease progression and prognostic factors. J
Hepatol 2008;48:335-52.
Nucleos(t)ide analogs provide excellent suppression of 19 Kurosaki M, Enomoto N, Asahina Y, et al. Mutations in the core promoter
HBV DNA and potential for regression of fibrosis but low region of hepatitis B virus in patients with chronic hepatitis B. J Med Virol
1996;49:115-23.
rates of HBeAg seroconversion and a high risk of relapse 20 Sato S, Suzuki K, Akahane Y, et al. Hepatitis B virus strains with mutations
after treatment is withdrawn. Monitoring of HBsAg values in the core promoter in patients with fulminant hepatitis. Ann Intern Med
1995;122:241-8.
can be used as a guide to response to therapy. Treatment 21 Chu CM, Lin CC, Chen YC, et al. Basal core promoter mutation is
aimed at alternative targets that may ultimately lead to a associated with progression to cirrhosis rather than hepatocellular
carcinoma in chronic hepatitis B virus infection. Br J Cancer
cure for HBV infection is currently under development. 2012;107:2010-5.
22 Liu CJ, Chen BF,Chen PJ, et al. Role of hepatitis B virus precore/core
Guidelines promoter mutations and serum viral load on noncirrhotic hepatocellular
carcinoma: a case-control study. J Infect Dis 2006;194:594-9.
HBV diagnosis and treatment guidelines are available 23 Liu CJ, Chen BF, Chen PJ, et al. Role of hepatitis B viral load and basal core
from the American Association for the Study of Liver Dis- promoter mutation in hepatocellular carcinoma in hepatitis B carriers. J
Infect Dis 2006;193:1258-65.
ease (2009; www.aasld.org), European Association for 24 Raimondo G, Allain JP, Brunetto MR, et al. Statements from the
the Study of Liver Diseases (2012; www.easl.eu), and the Taormina expert meeting on occult hepatitis B virus infection. J Hepatol
2008;49:652-7.
Asian Pacific Association for Study of the Liver (2012; 25 Cacciola I, Pollicino T,Squadrito G, et al. Occult hepatitis B virus
www.apasl.info). All guidelines are of high quality, and infection in patients with chronic hepatitis C liver disease. N Engl J Med
1999;341:22-6.
we have cited recommendations from these guidelines 26 Squadrito G, Cacciola I, Alibrandi A, et al. Impact of occult hepatitis B virus
on evaluation, treatment initiation, and management of infection on the outcome of chronic hepatitis C. J Hepatol 2013;59:696-
700.
antiviral resistance.
27 Gerlich WH, Glebe D, Schuttler CG. Deficiencies in the standardization
Contributors: VS and KK contributed equally to conceptualization and and sensitivity of diagnostic tests for hepatitis B virus. J Viral Hepatitis
study design, including literature search, and drafting and critical revision 2007;14(suppl 1):16-21.
of the manuscript. Both authors are guarantors. 28 Raimondo G, Pollicino T, Cacciola I, Squadrito G. Occult hepatitis B virus
Competing interests: We have read and understood BMJ policy on infection. J Hepatol 2007;46:160-70.
29 Lai M, Hyatt BJ, Nasser I, et al. The clinical significance of persistently
declaration of interests and declare the following interests: VS: speakers
normal ALTin chronic hepatitis B infection. J Hepatol 2007;47:760-7.
bureau: Salix (makes no products related to this review and has no
30 Chao DT, Lim JK, Ayoub WS, et al. Systematic review with meta-analysis:
relationship to the subject matter); advisory board: Gilead, Abbvie, Janssen. the proportion of chronic hepatitis B patients with normal alanine
KK: grants/research: Evidera, Gilead, Immuron, Intercept, Tobira; advisory transaminase ≤40 IU/L and significant hepatic fibrosis. Aliment
board: Abbvie, Achillion, BMS, Evidera, Gilead, Merck, Novartis, Trio Health; Pharmacol Ther 2014;39:349-58.
consultant: Abbvie, Gilead. 31 Rockey DC, Caldwell SH, Goodman ZD, et al; American Association for the
Provenance and peer review: Commissioned; externally peer reviewed. Study of Liver Diseases. Liver biopsy. Hepatology 2009;49:1017-44.
For personal use only 10 of 12
STATE OF THE ART REVIEW
32 Wai CT, Greenson JK, Fontana RJ, et al. A simple noninvasive index can 63 Chang TT, Lai CL, Kew Yoon S, et al. Entecavir treatment for up to 5 years
predict both significant fibrosis and cirrhosis in patients with chronic in patients with hepatitis B e antigen-positive chronic hepatitis B.
hepatitis C. Hepatology 2003;38:518-26. Hepatology 2010;51:422-30.
33 Sterling RK, Lissen E, Clumeck N, et al. Development of a simple 64 Tenney DJ, Rose RE, Baldick CJ, et al. Long-term monitoring shows
noninvasive index to predict significant fibrosis in patients with HIV/HCV hepatitis B virus resistance to entecavir in nucleoside-naive patients is
coinfection. Hepatology 2006;43:1317-25. rare through 5 years of therapy. Hepatology 2009;49:1503-14.
34 Xiao G, Yang J, Yan L. Comparison of diagnostic accuracy of aspartate 65 Yuen MF, Seto WK, Fung J, Wong DK, Yuen JC, Lai CL. Three years of
aminotransferase to platelet ratio index and fibrosis-4 index for detecting continuous entecavir therapy in treatment-naive chronic hepatitis B
liver fibrosis in adult patients with chronic hepatitis B virus infection: a patients: VIRAL suppression, viral resistance, and clinical safety. Am J
systemic review and meta-analysis. Hepatology 2015;61:292-302. Gastroenterol 2011;106:1264-71.
35 Yeh WC, Li PC, Jeng YM, et al. Elastic modulus measurements of human liver 66 Lange CM, Bojunga J, Hofmann WP, et al. Severe lactic acidosis during
and correlation with pathology. Ultrasound Med Biol 2002;28:467-74. treatment of chronic hepatitis B with entecavir in patients with impaired
36 Colombo S, Belloli L, Zaccanelli M, et al. Normal liver stiffness and its liver function. Hepatology 2009;50:2001-6.
determinants in healthy blood donors. Dig Liver Dis 2011;43:231-6. 67 Liaw YF,Sheen IS, Lee CM, et al. Tenofovir disoproxil fumarate (TDF),
37 Kim SU, Choi GH, Han WK, et al. What are “true normal” liver stiffness emtricitabine/TDF, and entecavir in patients with decompensated chronic
values using FibroScan? A prospective study in healthy living liver and hepatitis B liver disease. Hepatology 2011;53:62-72.
kidney donors in South Korea. Liver Int 2010;30:268-74. 68 Shim JH, Lee HC, Kim KM, et al. Efficacy of entecavir in treatment-naive
38 Roulot D, Czernichow S, Le Clesiau H et al. Liver stiffness values in patients with hepatitis B virus-related decompensated cirrhosis. J Hepatol
apparently healthy subjects: influence of gender and metabolic 2010;52:176-82.
syndrome. J Hepatol 2008;48:606-13. 69 Marcellin P,Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate
39 Marcellin P, Ziol M, Bedossa P, et al. Non-invasive assessment of liver versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med
fibrosis by stiffness measurement in patients with chronic hepatitis B. 2008;359:2442-55.
Liver Int 2009;29:242-7. 70 Corsa AC, Liu Y, Flaherty JF, et al. No detectable resistance to tenofovir
40 Friedrich-Rust M, Ong MF, Martens S, et al. Performance of transient disoproxil fumarate (TDF) in HBeAg+ and HBeAg− patients with chronic
elastography for the staging of liver fibrosis: a meta-analysis. hepatitis B (CHB) after eight years of treatment. Hepatology 2014;1707.
Gastroenterology 2008;134:960-74. 71 Lok AS, Trinh H, Carosi G, et al. Efficacy of entecavir with or without
41 Chon YE, Choi EH, Song KJ, et al. Performance of transient elastography tenofovir disoproxil fumarate for nucleos(t)ide-naive patients with chronic
for the staging of liver fibrosis in patients with chronic hepatitis B: a meta- hepatitis B. Gastroenterology 2012;143:619-28 e1.
analysis. PloS One 2012;7:e44930. 72 Fung S, Kwan P,Fabri M, et al. Randomized comparison of tenofovir
42 Jonas MM, Block JM, Haber BA, et al. Treatment of children with chronic disoproxil fumarate vs emtricitabine and tenofovir disoproxil fumarate in
hepatitis B virus infection in the United States: patient selection and patients with lamivudine-resistant chronic hepatitis B. Gastroenterology
therapeutic options. Hepatology 2010;52:2192-205. 2014;146:980-8.
43 Chan HL, Chan CK, Hui AJ, et al. Effects of tenofovir disoproxil fumarate 73 Van Bommel F,de Man RA, Wedemeyer H, et al. Long-term efficacy of
in hepatitis B e antigen-positive patients with normal levels of tenofovir monotherapy for hepatitis B virus-monoinfected patients after
alanine aminotransferase and high levels of hepatitis B virus DNA. failure of nucleoside/nucleotide analogues. Hepatology 2010;51:73-80.
Gastroenterology 2014;146:1240-8. 74 Reijnders JG, Deterding K, Petersen J, et al. Antiviral effect of entecavir
44 Tong MJ, Trieu J. Hepatitis B inactive carriers: clinical course and in chronic hepatitis B: influence of prior exposure to nucleos(t)ide
outcomes. J Digest Dis 2013;14:311-7. analogues. J Hepatol 2010;52:493-500.
45 Chen JD, Yang HI, Iloeje UH, et al. Carriers of inactive hepatitis B virus 75 Lim YS, Byun KS, Yoo BC, et al. Tenofovir monotherapy versus tenofovir
are still at risk for hepatocellular carcinoma and liver-related death. and entecavir combination therapy in patients with entecavir-resistant
Gastroenterology 2010;138:1747-54. chronic hepatitis B with multiple drug failure: results of a randomised trial.
46 Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for Gut 2015.
serum alanine aminotransferase levels. Ann Intern Med 2002;137:1-10. 76 Deguchi M, Yamashita N, Kagita M, et al. Quantitation of hepatitis B
47 Chen CJ, Yang HI, Iloeje UH, et al. Hepatitis B virus DNA levels and surface antigen by an automated chemiluminescent microparticle
outcomes in chronic hepatitis B. Hepatology 2009;49:S72-84. immunoassay. J Virologic Methods 2004;115:217-22.
48 Iloeje UH, Yang HI, Su J, et al. Predicting cirrhosis risk based on the level of 77 Zacher BJ, Moriconi F, Bowden S, et al. Multicenter evaluation of the
circulating hepatitis B viral load. Gastroenterology 2006;130:678-86. Elecsys hepatitis B surface antigen quantitative assay. Clin Vaccine
49 Chen CJ, Yang HI, Su J, et al. Risk of hepatocellular carcinoma across Immunol 2011;18:1943-50.
a biological gradient of serum hepatitis B virus DNA level. JAMA 78 Honer Zu Siederdissen C, Cornberg M. The role of HBsAg levels in the
2006;295:65-73. current management of chronic HBV infection. Ann Gastroenterol
50 Chen CF, Lee WC, Yang HI, et al. Changes in serum levels of HBV DNA and 2014;27:105-12.
alanine aminotransferase determine risk for hepatocellular carcinoma. 79 Seto WK, Wong DK, Fung J, et al. High hepatitis B surface antigen levels
Gastroenterology 2011;141:1240-8, 8 e1-2. predict insignificant fibrosis in hepatitis B e antigen positive chronic
51 Feeney ER, Chung RT. Antiviral treatment of hepatitis C. BMJ hepatitis B. PloS One 2012;7:e43087.
2014;348:g3308. 80 Martinot-Peignoux M, Carvalho-Filho R, Lapalus M, et al. Hepatitis
52 Buster EH, Hansen BE, Lau GK, et al. Factors that predict response B surface antigen serum level is associated with fibrosis severity in
of patients with hepatitis B e antigen-positive chronic hepatitis B to treatment-naive, e antigen-positive patients. J Hepatol 2013;58:1089-
peginterferon-alfa. Gastroenterology 2009;137:2002-9. 95.
53 Santantonio TA, Fasano M. Chronic hepatitis B: Advances in treatment. 81 Brunetto MR, Oliveri F, Colombatto P, et al. Hepatitis B surface antigen
World J Hepatol 2014;6:284-92. serum levels help to distinguish active from inactive hepatitis B virus
54 Sonneveld MJ, Wong VW, Woltman AM, et al. Polymorphisms near IL28B genotype D carriers. Gastroenterology 2010;139:483-90.
and serologic response to peginterferon in HBeAg-positive patients with 82 Takkenberg RB, Jansen L, de Niet A, et al. Baseline hepatitis B surface
chronic hepatitis B. Gastroenterology 2012;142:513-20 e1. antigen (HBsAg) as predictor of sustained HBsAg loss in chronic hepatitis
55 Lau GK, Piratvisuth T, Luo KX, et al. Peginterferon alfa-2a, lamivudine, B patients treated with pegylated interferon-alpha2a and adefovir.
and the combination for HBeAg-positive chronic hepatitis B. N Engl J Med Antiviral Ther 2013;18:895-904.
2005;352:2682-95. 83 Chan HL, Wong VW, Chim AM, et al. Serum HBsAg quantification to predict
56 Marcellin P,Lau GK, Bonino F, et al. Peginterferon alfa-2a alone, response to peginterferon therapy of e antigen positive chronic hepatitis
lamivudine alone, and the two in combination in patients with HBeAg- B. Aliment Pharmacol Ther 2010;32:1323-31.
negative chronic hepatitis B. N Engl J Med 2004;351:1206-17. 84 Sonneveld MJ, Rijckborst V, Boucher CA, et al. Prediction of sustained
57 Rijckborst V, ter Borg MJ, Cakaloglu Y, et al. A randomized trial of response to peginterferon alfa-2b for hepatitis B e antigen-positive
peginterferon alpha-2a with or without ribavirin for HBeAg-negative chronic hepatitis B using on-treatment hepatitis B surface antigen
chronic hepatitis B. Am J Gastroenterol 2010;105:1762-9. decline. Hepatology 2010;52:1251-7.
58 Liaw YF, Jia JD, Chan HL, et al. Shorter durations and lower doses of 85 Moucari R, Mackiewicz V, Lada O, et al. Early serum HBsAg drop: a strong
peginterferon alfa-2a are associated with inferior hepatitis B e antigen predictor of sustained virological response to pegylated interferon alfa-2a
seroconversion rates in hepatitis B virus genotypes B or C. Hepatology in HBeAg-negative patients. Hepatology 2009;49:1151-7.
2011;54:1591-9. 86 Reijnders JG, Perquin MJ, Zhang N, et al. Nucleos(t)ide analogues only
59 Lampertico P, Vigano M, Di Costanzo GG, et al. Randomised study induce temporary hepatitis B e antigen seroconversion in most patients
comparing 48 and 96 weeks peginterferon alpha-2a therapy in genotype with chronic hepatitis B. Gastroenterology 2010;139:491-8.
D HBeAg-negative chronic hepatitis B. Gut 2013;62:290-8. 87 Lee HW, Lee HJ, Hwang JS, et al. Lamivudine maintenance beyond
60 Chang TT, Gish RG, de Man R, et al. A comparison of entecavir and one year after HBeAg seroconversion is a major factor for sustained
lamivudine for HBeAg-positive chronic hepatitis B. N Engl J Med virologic response in HBeAg-positive chronic hepatitis B. Hepatology
2006;354:1001-10. 2010;51:415-21.
61 Lai CL, Shouval D, Lok AS, et al. Entecavir versus lamivudine for patients 88 Hadziyannis SJ, Sevastianos V, Rapti I, et al. Sustained responses and loss
with HBeAg-negative chronic hepatitis B. N Engl J Med 2006;354:1011- of HBsAg in HBeAg-negative patients with chronic hepatitis B who stop
20. long-term treatment with adefovir. Gastroenterology 2012;143:629-36 e1.
62 Gish RG, Lok AS, Chang TT, et al. Entecavir therapy for up to 96 weeks 89 Seto WK, Hui AJ, Wong VW, et al. Treatment cessation of entecavir in
in patients with HBeAg-positive chronic hepatitis B. Gastroenterology Asian patients with hepatitis B e antigen negative chronic hepatitis B: a
2007;133:1437-44. multicentre prospective study. Gut 2015;64:667-72.
For personal use only 11 of 12
STATE OF THE ART REVIEW
90 Fontaine H, Kahi S, Chazallon C, et al. Anti-HBV DNA vaccination does 115 Pan CQ, Han GR, Jiang HX, et al. Telbivudine prevents vertical transmission
not prevent relapse after discontinuation of analogues in the treatment from HBeAg-positive women with chronic hepatitis B. Clin Gastroenterol
of chronic hepatitis B: a randomised trial-ANRS HB02 VAC-ADN. Gut Hepatol 2012;10:520-6.
2015;64:139-47. 116 Han GR, Cao MK, Zhao W, et al. A prospective and open-label study for
91 Marcellin P, Gane E, Buti M, et al. Regression of cirrhosis during treatment the efficacy and safety of telbivudine in pregnancy for the prevention
with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open- of perinatal transmission of hepatitis B virus infection. J Hepatol
label follow-up study. Lancet 2013;381:468-75. 2011;55:1215-21.
92 Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patients with chronic 117 Ehrhardt S, Xie C, Guo N, Nelson K, Thio CL. Breastfeeding while taking
hepatitis B and advanced liver disease. N Engl J Med 2004;351:1521-31. lamivudine or tenofovir disoproxil fumarate: a review of the evidence. Clin
93 Hosaka T, Suzuki F, Kobayashi M, et al. Long-term entecavir treatment Infect Dis 2015;60:275-8.
reduces hepatocellular carcinoma incidence in patients with hepatitis B 118 Hoofnagle JH. Reactivation of hepatitis B. Hepatology 2009;49:S156-65.
virus infection. Hepatology 2013;58:98-107. 119 Hwang JP, Lok AS. Management of patients with hepatitis B who
94 Wong GL, Chan HL, Mak CW, et al. Entecavir treatment reduces hepatic require immunosuppressive therapy. Nat Rev Gastroenterol Hepatol
events and deaths in chronic hepatitis B patients with liver cirrhosis. 2014;11:209-19.
Hepatology 2013;58:1537-47. 120 Vassilopoulos D, Calabrese LH. Management of rheumatic disease with
95 Wu CY, Lin JT, Ho HJ, et al. Association of nucleos(t)ide analogue therapy comorbid HBV or HCV infection. Nat Rev Rheumatol 2012;8:348-57.
with reduced risk of hepatocellular carcinoma in patients with chronic 121 Di Bisceglie AM, Lok AS, Martin P,et al. Recent US Food and Drug
hepatitis B: a nationwide cohort study. Gastroenterology 2014;147:143- Administration warnings on hepatitis B reactivation with immune-
51 e5. suppressing and anticancer drugs: just the tip of the iceberg? Hepatology
96 Papatheodoridis GV, Chan HL, Hansen BE, et al. Risk of hepatocellular 2015;61:703-11.
carcinoma in chronic hepatitis B: assessment and modification with 122 Reddy KR, Beavers KL, Hammond SP,et al. American gastroenterological
current antiviral therapy. J Hepatol 2015;62:956-67. association institute guideline on the prevention and treatment of
97 Phung BC, Sogni P, Launay O. Hepatitis B and human immunodeficiency hepatitis B virus reactivation during immunosuppressive drug therapy.
virus co-infection. World J Gastroenterol 2014;20:17360-7. Gastroenterology 2015;148:215-9.
98 McGovern BH. The epidemiology, natural history and prevention of 123 Lau GK, Yiu HH, Fong DY, et al. Early is superior to deferred preemptive
hepatitis B: implications of HIV coinfection. Antiviral Ther 2007;12(suppl lamivudine therapy for hepatitis B patients undergoing chemotherapy.
3):H3-13. Gastroenterology 2003;125:1742-9.
99 Thio CL. Hepatitis B and human immunodeficiency virus coinfection. 124 Hsu C, Hsiung CA, Su IJ, et al. A revisit of prophylactic lamivudine for
Hepatology 2009;49:S138-45. chemotherapy-associated hepatitis B reactivation in non-Hodgkin’s
100 Puoti M, Torti C, Bruno R, et al. Natural history of chronic hepatitis B in lymphoma: a randomized trial. Hepatology 2008;47:844-53.
co-infected patients. J Hepatol 2006;44:S65-70. 125 Saab S, Dong MH, Joseph TA, et al. Hepatitis B prophylaxis in patients
101 Thio CL, Seaberg EC, Skolasky R, Jr., et al. HIV-1, hepatitis B virus, and risk undergoing chemotherapy for lymphoma: a decision analysis model.
of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet Hepatology 2007;46:1049-56.
2002;360:1921-6. 126 Huang YH, Hsiao LT,Hong YC, et al. Randomized controlled trial of
102 Konopnicki D, Mocroft A, de Wit S, et al. Hepatitis B and HIV: prevalence, entecavir prophylaxis for rituximab-associated hepatitis B virus
AIDS progression, response to highly active antiretroviral therapy and reactivation in patients with lymphoma and resolved hepatitis B. J Clin
increased mortality in the EuroSIDA cohort. AIDS 2005;19:593-601. Oncol 2013;31:2765-72.
103 Benhamou Y, Fleury H, Trimoulet P, et al. Anti-hepatitis B virus efficacy 127 Hsu C, Tsou HH, Lin SJ, et al. Chemotherapy-induced hepatitis B
of tenofovir disoproxil fumarate in HIV-infected patients. Hepatology reactivation in lymphoma patients with resolved HBV infection: a
2006;43:548-55. prospective study. Hepatology 2014;59:2092-100.
104 Price H, Dunn D, Pillay D, et al. Suppression of HBV by tenofovir in HBV/ 128 Jayalakshmi MMK, Kalyanaraman N, Pitchappan R. Hepatitis B virus
HIV coinfected patients: a systematic review and meta-analysis. PloS One genetic diversity: disease pathogenesis, viral replication. In: Rosas-Acosta
2013;8:e68152. G, ed. Immunology and microbiology “viral replication.” InTech, 2013.
105 Noureddin M, Gish R. Hepatitis delta: epidemiology, diagnosis www.intechopen.com/books/viral-replication/hepatitis-b-virus-genetic-
and management 36 years after discovery. Curr Gastroenterol Rep diversity-disease-pathogenesis.
2014;16:365. 129 Kapoor R, Kottilil S. Strategies to eliminate HBV infection. Future Virol
106 Wedemeyer H, Yurdaydin C, Dalekos GN, et al. Peginterferon plus 2014;9:565-85.
adefovir versus either drug alone for hepatitis delta. N Engl J Medic 130 Wang XY,Chen HS. Emerging antivirals for the treatment of hepatitis B.
2011;364:322-31. World J Gastroenterol 2014;20:7707-17.
107 Heidrich B, Yurdaydin C, Kabacam G, et al. Late HDV RNA relapse after 131 Petersen J, Dandri M, Mier W, et al. Prevention of hepatitis B virus infection
peginterferon alpha-based therapy of chronic hepatitis delta. Hepatology in vivo by entry inhibitors derived from the large envelope protein. Nat
2014;60:87-97. Biotechnol 2008;26:335-41.
108 Wedermeyer H, Yurdaydin C, Ernst S, et al. Prolonged therapy of hepatitis 132 Volz T, Allweiss L, Ben MM, et al. The entry inhibitor myrcludex-B efficiently
delta for 96 weeks with pegylated-interferon-a-2a plus tenofovir or blocks intrahepatic virus spreading in humanized mice previously
placebo does not prevent HDV RNA relapse after treatment: the HIDIT-2 infected with hepatitis B virus. J Hepatol 2013;58:861-7.
study. 49th European Association for the Study of the Liver International 133 Stray SJ, Zlotnick A. BAY 41-4109 has multiple effects on Hepatitis B virus
Liver Congress (EASL 2014). London, April 9-13, 2014. Abstract O4. capsid assembly. J Mol Recogn 2006;19:542-8.
http://hepatitis-delta.org/assets/DownloadPage/000000/2014-04- 134 Wang XY, Wei ZM, Wu GY, et al. In vitro inhibition of HBV replication by
HIDIT-II-EASL-Homepage.pdf. a novel compound, GLS4, and its efficacy against adefovir-dipivoxil-
109 Patton H, Tran TT. Management of hepatitis B during pregnancy. Nat Rev resistant HBV mutations. Antiviral Ther 2012;17:793-803.
Gastroenterol Hepatol 2014;11:402-9. 135 Mahtab MA, Bazinet M, Patient R, et al. REP 9 AC: a potent HBsAg release
110 US Department of Health and Human Services. MMWR: a comprehensive inhibitor that elicits durable immunological control of chronic HBV
immunization strategy to eliminate transmission of hepatitis B virus infection. Hepatology 2011;54(suppl S1): 478A.
infection in the United States. 2005. www.cdc.gov/mmwr/preview/ 136 Lanford RE, Guerra B, Chavez D, et al. GS-9620, an oral agonist of Toll-
mmwrhtml/rr5416a1.htm. like receptor-7, induces prolonged suppression of hepatitis B virus in
111 Zou H, Chen Y, Duan Z, et al. Virologic factors associated with failure to chronically infected chimpanzees. Gastroenterology 2013;144:1508-17,
passive-active immunoprophylaxis in infants born to HBsAg-positive 17 e1-10.
mothers. J Viral Hepatitis 2012;19:e18-25. 137 Spellman M, Martin JT. Treatment of chronic hepatitis B infection with
112 Shaheen AA, Myers RP. The outcomes of pregnancy in patients with DV-601, a therapeutic vaccine. J Hepatol 2011;54(suppl 1):s302.
cirrhosis: a population-based study. Liver Int 2010;30:275-83. 138 Zimmerman KA, Fischer KP, Joyce MA, et al. Zinc finger proteins designed
113 Peginterferon alfa-2b pregnancy and breastfeeding warnings. www.drugs. to specifically target duck hepatitis B virus covalently closed circular DNA
com/pregnancy/peginterferon-alfa-2b.html. inhibit viral transcription in tissue culture. J Virol 2008;82:8013-21.
114 Pan CQ, Mi LJ, Bunchorntavakul C, et al. Tenofovir disoproxil fumarate for 139 CaiD, Mills C, Yu W,et al. Identification of disubstituted sulfonamide
prevention of vertical transmission of hepatitis B virus infection by highly compounds as specific inhibitors of hepatitis B virus covalently closed
viremic pregnant women: a case series. Dig Dis Sci 2012;57:2423-9. circular DNA formation. Antimicrob Agents Chemother 2012;56:4277-88.
For personal use only 12 of 12
You might also like
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Health Care Market ObjectivesDocument18 pagesHealth Care Market ObjectivesChris Ian AgustinNo ratings yet
- Lecture I Anatomy of The Gi Tract Lecture Notes Lectures 1 20 PDFDocument322 pagesLecture I Anatomy of The Gi Tract Lecture Notes Lectures 1 20 PDFLilyNo ratings yet
- Development of The Urinary SystemDocument36 pagesDevelopment of The Urinary SystemAmanuel MaruNo ratings yet
- 3rd Edition Self-Assessment in Respiratory MedicineDocument267 pages3rd Edition Self-Assessment in Respiratory MedicineamjadsabahNo ratings yet
- Atrial Fibrillation: Bibek Raj Poudel Intern Pahs-SomDocument34 pagesAtrial Fibrillation: Bibek Raj Poudel Intern Pahs-SomKishor K AdhikariNo ratings yet
- UTIDocument17 pagesUTIBongkotchakorn Mind PhonchaiNo ratings yet
- Dr. Arlene Jane Sy-Reodica Clinical Applications Specialist - ASEAN Monitoring SolutionsDocument43 pagesDr. Arlene Jane Sy-Reodica Clinical Applications Specialist - ASEAN Monitoring SolutionsArNo ratings yet
- Metheny - Fluid and Electrolyte Balance 4th EdDocument227 pagesMetheny - Fluid and Electrolyte Balance 4th Edfirst aid kit100% (1)
- Clinical Biochemistry HSST CurriculumDocument111 pagesClinical Biochemistry HSST CurriculumChengyuan ZhangNo ratings yet
- ICD 10 CM ConversionTable FY17Document92 pagesICD 10 CM ConversionTable FY17Ernes PutraNo ratings yet
- (Journal) Clinical Pharmacology Therapeutics Journal. Volume 85. Issue 5 (2009) PDFDocument111 pages(Journal) Clinical Pharmacology Therapeutics Journal. Volume 85. Issue 5 (2009) PDFRicovially DavyaNo ratings yet
- Queen's Medical Review 5.2Document28 pagesQueen's Medical Review 5.2Queen's Medical Review100% (1)
- Beta BlockersDocument70 pagesBeta BlockersIrina Cabac-PogoreviciNo ratings yet
- IV Fluid ManagementDocument10 pagesIV Fluid ManagementNararto PrijogoNo ratings yet
- Elective BookDocument236 pagesElective BookAbdullahNo ratings yet
- Slides of Fever 3Document52 pagesSlides of Fever 3Selly SelNo ratings yet
- Point of Care Testing Policy Guideline: Edition 1: 2016Document40 pagesPoint of Care Testing Policy Guideline: Edition 1: 2016Paul100% (1)
- MedSciPostgrad PDFDocument113 pagesMedSciPostgrad PDFCarlyle MarinNo ratings yet
- Ch221 Class 8 Chapter 4: Stereochemistry of Alkanes and Cycloalkanes, ContinuedDocument11 pagesCh221 Class 8 Chapter 4: Stereochemistry of Alkanes and Cycloalkanes, ContinuedSanjay Mani TripathiNo ratings yet
- Phase I Handbook - MBBS Programme - University of BotswanaDocument43 pagesPhase I Handbook - MBBS Programme - University of BotswanaNil NilNo ratings yet
- Fluid and Electrolyte Imbalance in Heart Attack PatientDocument3 pagesFluid and Electrolyte Imbalance in Heart Attack Patientroy_linaoNo ratings yet
- Acid Base Equilibrium, Clinical Concepts and Acid Base DisordersDocument64 pagesAcid Base Equilibrium, Clinical Concepts and Acid Base DisordersevanNo ratings yet
- GERIATRIC MEDICINE (Basic)Document41 pagesGERIATRIC MEDICINE (Basic)Medical AdvicesNo ratings yet
- Clinical Handover Ian ScottDocument26 pagesClinical Handover Ian ScottYwagar YwagarNo ratings yet
- NHO Code of Practice For Healthcare Records Management Version 2 0Document370 pagesNHO Code of Practice For Healthcare Records Management Version 2 0Khirod SahuNo ratings yet
- Medical Statistics Made Easy For The Medical Pract PDFDocument6 pagesMedical Statistics Made Easy For The Medical Pract PDFDragomir P. AdrianNo ratings yet
- Guidelines For SB and U5 Mortality Reporting System 2nd Edition 2018Document24 pagesGuidelines For SB and U5 Mortality Reporting System 2nd Edition 2018Roziha RahimNo ratings yet
- Defects and Donuts: The Importance of The Mesh:defect Area RatioDocument3 pagesDefects and Donuts: The Importance of The Mesh:defect Area RatioGuille PuertasNo ratings yet
- Concept of Statistical Quality ControlDocument51 pagesConcept of Statistical Quality ControlTehmeena BegumNo ratings yet
- Acute HD Prescription GuideDocument24 pagesAcute HD Prescription GuideSurya Abadi KristyoadiNo ratings yet
- TEMPLATE Clinical Reasoning Case Study2Document10 pagesTEMPLATE Clinical Reasoning Case Study2Ianne MerhNo ratings yet
- MSC - Biomedical - Sciences Programme Spec 2012 EntryDocument4 pagesMSC - Biomedical - Sciences Programme Spec 2012 EntryNELSON NWANOKENo ratings yet
- Value and Quality Innovations in Acute and Emergency CareDocument246 pagesValue and Quality Innovations in Acute and Emergency CareHas MasNo ratings yet
- Juran's Quality Improvement ProcessDocument68 pagesJuran's Quality Improvement Processyousrazeidan1979No ratings yet
- H&P GuideDocument7 pagesH&P GuideTBWPNo ratings yet
- GDC Maintaining Standards GuidanceDocument90 pagesGDC Maintaining Standards GuidanceSara Loureiro da LuzNo ratings yet
- Clinical Management of COVID-19 - V7Document59 pagesClinical Management of COVID-19 - V7Natalia VelandiaNo ratings yet
- Blood Flow Q: The Transmembrane Pressure (TMP) GradientDocument1 pageBlood Flow Q: The Transmembrane Pressure (TMP) GradientNicholas HelmstetterNo ratings yet
- Clinical practice guidelines critical appraisal guideDocument2 pagesClinical practice guidelines critical appraisal guideWijitha VarenniNo ratings yet
- Hemoptysis 1Document27 pagesHemoptysis 1Aida SiregarNo ratings yet
- Barna Standards of Practice 2012Document42 pagesBarna Standards of Practice 2012evangelinaNo ratings yet
- Critical Care Cardiovascular Disease Chapter 22: Classification, Pathophysiology, and Management of ShockDocument44 pagesCritical Care Cardiovascular Disease Chapter 22: Classification, Pathophysiology, and Management of Shockismi latifahNo ratings yet
- Stroke: AHA/ASA Guidelines For The Early Management of Patients With Acute Ischemic Stroke (2019)Document14 pagesStroke: AHA/ASA Guidelines For The Early Management of Patients With Acute Ischemic Stroke (2019)Natalia OrtizNo ratings yet
- A Guide To Common Blood TestsDocument3 pagesA Guide To Common Blood TestsshahjituNo ratings yet
- Noac GuidelinesDocument40 pagesNoac GuidelinesCocosul Cocosului CocosaruluiNo ratings yet
- Proximal Versus Total Gastrectomy For - Proximal GastricDocument11 pagesProximal Versus Total Gastrectomy For - Proximal GastricMario CeaNo ratings yet
- Measuring Patient Safety Attitudes, Skills and KnowledgeDocument5 pagesMeasuring Patient Safety Attitudes, Skills and KnowledgeEko Wahyu AgustinNo ratings yet
- JChiroprHumanit2007v14 34-40 PDFDocument7 pagesJChiroprHumanit2007v14 34-40 PDFRetno SawitriNo ratings yet
- Rheumtatic Fever 2018Document63 pagesRheumtatic Fever 2018shapan biswaNo ratings yet
- Johsnson N JohnsonDocument10 pagesJohsnson N JohnsonJyotiNo ratings yet
- Interstitial Lung Disease Diagnosis and TreatmentDocument23 pagesInterstitial Lung Disease Diagnosis and TreatmentNogra CarlNo ratings yet
- PHARMAKOKINETICSDocument16 pagesPHARMAKOKINETICSGauthaman KarunakaranNo ratings yet
- Hospital Wards and Departments GuideDocument35 pagesHospital Wards and Departments GuideSerendipity English100% (1)
- Handbook of Anticancer Pharmacokinetics and Pharmacodynamics 2004Document623 pagesHandbook of Anticancer Pharmacokinetics and Pharmacodynamics 2004Harsh KoshtiNo ratings yet
- Lab Flow SheetDocument2 pagesLab Flow SheetRyan LazatinNo ratings yet
- Tubes, Lines, and Drains Basics: Harmacy Ompetency Ssessment EnterDocument11 pagesTubes, Lines, and Drains Basics: Harmacy Ompetency Ssessment EnterJeremy HamptonNo ratings yet
- Aga Khan University Postgraduate Medical Education (Pgme) Induction Frequently Asked QuestionsDocument12 pagesAga Khan University Postgraduate Medical Education (Pgme) Induction Frequently Asked QuestionsYasir QureshiNo ratings yet
- CPG Unstable AnginaDocument58 pagesCPG Unstable AnginaAmir HassenNo ratings yet
- Jurnal 3Document6 pagesJurnal 3rifahNo ratings yet
- EpidemioDocument1 pageEpidemiorifahNo ratings yet
- Jurnal 1Document7 pagesJurnal 1rifahNo ratings yet
- Coulm Et al-2015-BJOG An International Journal of Obstetrics & GynaecologyDocument7 pagesCoulm Et al-2015-BJOG An International Journal of Obstetrics & GynaecologyrifahNo ratings yet
- CitokinDocument1 pageCitokinrifahNo ratings yet
- Coulm Et al-2015-BJOG An International Journal of Obstetrics & GynaecologyDocument7 pagesCoulm Et al-2015-BJOG An International Journal of Obstetrics & GynaecologyrifahNo ratings yet
- Epilepsy Guideline ST Epilepticus Children N Adult 2016Document14 pagesEpilepsy Guideline ST Epilepticus Children N Adult 2016Desi ChiloupChaNo ratings yet
- Bor Et al-2016-BJOG An International Journal of Obstetrics & GynaecologyDocument7 pagesBor Et al-2016-BJOG An International Journal of Obstetrics & GynaecologyrifahNo ratings yet
- Jurnal 1Document7 pagesJurnal 1rifahNo ratings yet
- Clinical Practice Guidelines for Hepatitis B Virus (HBV) ManagementDocument48 pagesClinical Practice Guidelines for Hepatitis B Virus (HBV) ManagementAqila MumtazNo ratings yet
- Management of chronic hepatitis B infectionDocument12 pagesManagement of chronic hepatitis B infectionrifahNo ratings yet
- Hal 7Document1 pageHal 7rifahNo ratings yet
- Cipla Product ListDocument33 pagesCipla Product ListSumit Singhania100% (2)
- Penatalaksanaan Sirosis Hati dan HepatitisDocument14 pagesPenatalaksanaan Sirosis Hati dan HepatitisIrene Andriani HalimNo ratings yet
- Baraclude™ (Entecavir) Baraclude™ (Entecavir) Tablets Baraclude™ (Entecavir) Oral SolutionDocument25 pagesBaraclude™ (Entecavir) Baraclude™ (Entecavir) Tablets Baraclude™ (Entecavir) Oral SolutiondrchughNo ratings yet
- Drug Study EntecavirDocument4 pagesDrug Study EntecavirClarimae AwingNo ratings yet
- Tacke2016 - Treatment For Hepatitis B in Patients With Drug ResistanceDocument7 pagesTacke2016 - Treatment For Hepatitis B in Patients With Drug ResistanceClarisa AnindyaNo ratings yet
- HBVGuidance Terrault Et Al-2018-Hepatology PDFDocument40 pagesHBVGuidance Terrault Et Al-2018-Hepatology PDFAnonymous wdmpgxNo ratings yet
- Treatment Algorithm For Managing Chronic Hepatitis B VirusDocument10 pagesTreatment Algorithm For Managing Chronic Hepatitis B VirusRadhaRajasekaranNo ratings yet
- Bristol-Myers Squibb Company v. Apotex Et. Al.Document9 pagesBristol-Myers Squibb Company v. Apotex Et. Al.PriorSmartNo ratings yet
- Hepb Evidence ReportDocument671 pagesHepb Evidence ReportHerly Maulida SurdhawatiNo ratings yet
- Clinical guidelines for liver transplantationDocument53 pagesClinical guidelines for liver transplantationMadalina StoicescuNo ratings yet
- Bristol-Myers Squibb Company v. SandozDocument8 pagesBristol-Myers Squibb Company v. SandozPriorSmartNo ratings yet
- 2018 Management of Hepatitis BDocument13 pages2018 Management of Hepatitis BCamboy D' JablezNo ratings yet
- Baraclude: Generic Name: Entecavir 0.5 MG PO OD Antiviral AgentDocument8 pagesBaraclude: Generic Name: Entecavir 0.5 MG PO OD Antiviral AgentPatricia Jean FaeldoneaNo ratings yet
- Robert G. Gish, MD CV - May 2014Document221 pagesRobert G. Gish, MD CV - May 2014Robert G. Gish, MDNo ratings yet
- CKD Product - BD PackageDocument33 pagesCKD Product - BD PackageAhmedNo ratings yet
- Gish CV July 23 2014Document225 pagesGish CV July 23 2014Robert G. Gish, MDNo ratings yet
- CHRONIC HEPATITIS B SEROLOGY AND TREATMENTDocument28 pagesCHRONIC HEPATITIS B SEROLOGY AND TREATMENTVincent ReyesNo ratings yet
- Concept Map On HepatitisDocument1 pageConcept Map On HepatitisLaiNo ratings yet
- Hepatitis BDocument23 pagesHepatitis BAbraham RumayaraNo ratings yet
- Gish Publishing Activity 2013 - 2014Document8 pagesGish Publishing Activity 2013 - 2014Robert G. Gish, MDNo ratings yet
- Entecavir Patent Evaluation, Method For Diastereomeric Impurities OMCIJ - MS.ID.555711Document16 pagesEntecavir Patent Evaluation, Method For Diastereomeric Impurities OMCIJ - MS.ID.555711Drkrishnasarma pathyNo ratings yet
- Robert G Gish CV October 2014Document228 pagesRobert G Gish CV October 2014Robert G. Gish, MDNo ratings yet
- Zydus Cadila: Company Overview and Regulatory PositionDocument26 pagesZydus Cadila: Company Overview and Regulatory PositionRupam KunduNo ratings yet
- Drug study on Lamivudine, Entecavir, Milk Thistle, and Interferon AlfaDocument4 pagesDrug study on Lamivudine, Entecavir, Milk Thistle, and Interferon Alfaunyokies100% (1)
- Hepatite B CoinfeçãoDocument31 pagesHepatite B Coinfeçãojefferson2392No ratings yet
- Viral Hepatitis: Anatomy, Histology, Pathophysiology, Diagnosis, and TreatmentDocument46 pagesViral Hepatitis: Anatomy, Histology, Pathophysiology, Diagnosis, and TreatmentlubnaNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofWinnie WiyonoNo ratings yet
- Hepatitis B Cases StudiesDocument53 pagesHepatitis B Cases Studiesrieza_huseinNo ratings yet
- Hep v60 Is2 Rev1 Final 0Document1,283 pagesHep v60 Is2 Rev1 Final 0Marcela MurafaNo ratings yet
- Hepatitis B: The Immaculate Infection: Annmarie Huysman, MD Mitul Patel, MD Douglas T. Dieterich, MDDocument7 pagesHepatitis B: The Immaculate Infection: Annmarie Huysman, MD Mitul Patel, MD Douglas T. Dieterich, MDEnwunlu Bosso ThomasNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityFrom EverandThe Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityRating: 4.5 out of 5 stars4.5/5 (109)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)