You might also like
- Amohammaditofigh,+78 Jlms 35101Document10 pagesAmohammaditofigh,+78 Jlms 35101Lucas S. CostaNo ratings yet
- The Effectiveness of Therapeutic Class IV (10 W) Laser Treatment For EpicondylitisDocument7 pagesThe Effectiveness of Therapeutic Class IV (10 W) Laser Treatment For EpicondylitisDeborah SalinasNo ratings yet
- The Biomedical Effects of Laser ApplicationDocument9 pagesThe Biomedical Effects of Laser ApplicationSam SonNo ratings yet
- Low-Level Laser Therapy For Wound Healing: Mechanism and EfficacyDocument7 pagesLow-Level Laser Therapy For Wound Healing: Mechanism and EfficacyKarReséndizNo ratings yet
- Clinical and Histological Evaluation CO2Document10 pagesClinical and Histological Evaluation CO2BoeroNo ratings yet
- Prospective, Comparative Evaluation of Three Laser Systems Used Individually and in Combination For Axillary Hair RemovalDocument7 pagesProspective, Comparative Evaluation of Three Laser Systems Used Individually and in Combination For Axillary Hair RemovalmahsaNo ratings yet
- (03241750 - Acta Medica Bulgarica) Superluminous Devices Versus Low-Level Laser For Temporomandibular DisordersDocument5 pages(03241750 - Acta Medica Bulgarica) Superluminous Devices Versus Low-Level Laser For Temporomandibular DisordersTeodorNo ratings yet
- Full Thickness Wound Healing in Induced Diabetic Mice Using Low Level Laser in Comparison With UltrasoundDocument9 pagesFull Thickness Wound Healing in Induced Diabetic Mice Using Low Level Laser in Comparison With UltrasoundAnonymous UXBSV13cNo ratings yet
- Radiation Oncology A Physicists Eye ViewDocument332 pagesRadiation Oncology A Physicists Eye Viewquyen2012100% (1)
- Evaluation of An Ablative and Non-Ablative Laser Procedure in The Treatment of Striae Distensae 2014Document6 pagesEvaluation of An Ablative and Non-Ablative Laser Procedure in The Treatment of Striae Distensae 2014Paula GuimaNo ratings yet
- Radiotherapy: Basic Concepts and Recent AdvancesDocument17 pagesRadiotherapy: Basic Concepts and Recent AdvancesutokaNo ratings yet
- Wound Heling AmperageDocument8 pagesWound Heling AmperagegamalramadiNo ratings yet
- LLLT in Hair GrowthDocument13 pagesLLLT in Hair GrowthCarlos SilvaNo ratings yet
- Laser tissue interactions and potential onychomycosis therapyDocument4 pagesLaser tissue interactions and potential onychomycosis therapyJason BaumgardnerNo ratings yet
- Profundidade Laser 2012Document7 pagesProfundidade Laser 2012Josie ResendeNo ratings yet
- Topic 4Document3 pagesTopic 4Rabia BagewadiNo ratings yet
- ThongotherDocument6 pagesThongotherMarsella SetiawanNo ratings yet
- Effect of Low-Level Laser Therapy Burn Ulcer (Randomized Trial) PDFDocument5 pagesEffect of Low-Level Laser Therapy Burn Ulcer (Randomized Trial) PDFTatiana SiqueiraNo ratings yet
- Gentle Family: Laser SystemsDocument26 pagesGentle Family: Laser SystemsIgorNo ratings yet
- 4T3 Radiation TherapyDocument43 pages4T3 Radiation TherapydanaNo ratings yet
- Ji-Hye Park2019Document9 pagesJi-Hye Park2019Naiadja Santana CerqueiraNo ratings yet
- Medicina 59 00841Document7 pagesMedicina 59 00841maryellensprengerNo ratings yet
- Effectiveness of Low Intensity Laser Therapy On TH PDFDocument5 pagesEffectiveness of Low Intensity Laser Therapy On TH PDFBambang Ulan AeiyuNo ratings yet
- Ijerph 19 00801Document9 pagesIjerph 19 00801satriaNo ratings yet
- Censabella 2016Document9 pagesCensabella 2016Naiadja Santana CerqueiraNo ratings yet
- The Effects of Different Laser Doses OnDocument8 pagesThe Effects of Different Laser Doses OnАркадий ЖивицаNo ratings yet
- Randeberg 2007Document11 pagesRandeberg 2007Irvin MarcelNo ratings yet
- Radiation Therapy Toxicity To The Skin Derm Clin 2008Document12 pagesRadiation Therapy Toxicity To The Skin Derm Clin 2008Ana Karina Alvarado OsorioNo ratings yet
- Chapter 030Document2 pagesChapter 030Zaid juttNo ratings yet
- Role of Shortwave and MWD of CTSDocument11 pagesRole of Shortwave and MWD of CTSGaluh KurniasihNo ratings yet
- Low Level Laser Therapy: Healing at The Speed of LightDocument24 pagesLow Level Laser Therapy: Healing at The Speed of LightcumbredinNo ratings yet
- Review Laser Ablation For Cancer: Past, Present and FutureDocument15 pagesReview Laser Ablation For Cancer: Past, Present and FutureSujin JiracheewanunNo ratings yet
- Radiofrequency in Cosmetic Dermatology: Recent and Future DevelopmentsDocument10 pagesRadiofrequency in Cosmetic Dermatology: Recent and Future DevelopmentsNimade IndriNo ratings yet
- AlexandriteDocument4 pagesAlexandriteHong Nguyen ThiNo ratings yet
- The Biomedical Engineering Handbook: Second EditionDocument8 pagesThe Biomedical Engineering Handbook: Second Editionშაქრო ტრუბეცკოიNo ratings yet
- Journal Homepage: - : IntroductionDocument2 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Radiobiology Essentials for Medical ImagingDocument3 pagesRadiobiology Essentials for Medical ImagingdonnaNo ratings yet
- Study of The Ablative Effects of Nd:YAG or Er:YAG Laser RadiationDocument3 pagesStudy of The Ablative Effects of Nd:YAG or Er:YAG Laser RadiationdigdouwNo ratings yet
- 315 Rothkamm2012PLoSOne PDFDocument6 pages315 Rothkamm2012PLoSOne PDFKai RothkammNo ratings yet
- Subcutaneous Adipose Tissue Response To A Non-InvasiveDocument10 pagesSubcutaneous Adipose Tissue Response To A Non-InvasiveErik BrooksNo ratings yet
- Ke et al. - 2015 - ErYAG laser treatment stimulates hair growth through upregulating Wnt 10b and β-catenin expression in C57BL6 miceDocument7 pagesKe et al. - 2015 - ErYAG laser treatment stimulates hair growth through upregulating Wnt 10b and β-catenin expression in C57BL6 miceNicolás FarkasNo ratings yet
- 4 Radiobiology of Brachytherapy and The Dose-Rate EffectDocument27 pages4 Radiobiology of Brachytherapy and The Dose-Rate EffectDiana MitreaNo ratings yet
- Interstitial Laser Thermotherapy For Liver TumorsDocument15 pagesInterstitial Laser Thermotherapy For Liver TumorsSujin JiracheewanunNo ratings yet
- Quality Control of Ionizing Radiation in RadiotherapyDocument20 pagesQuality Control of Ionizing Radiation in RadiotherapyEskadmas BelayNo ratings yet
- Laser BiostimulationDocument4 pagesLaser BiostimulationzxoncoNo ratings yet
- Al Dhalimi2013Document6 pagesAl Dhalimi2013deltanueveNo ratings yet
- Comparison of Different Technologies For Non-Invasive Skin TighteningDocument9 pagesComparison of Different Technologies For Non-Invasive Skin TighteningThe Vancouver SunNo ratings yet
- Cancer ScanDocument10 pagesCancer ScanAngel MalzoneNo ratings yet
- Electron Beam Total Skin Irradiation PDFDocument1 pageElectron Beam Total Skin Irradiation PDFVictorM.LópezGuadalupeNo ratings yet
- Zaresharifi 2021Document7 pagesZaresharifi 2021abdulariifNo ratings yet
- Total Skin Electron Therapy: Technique and Dosimetry: Aapm Report No. 23Document58 pagesTotal Skin Electron Therapy: Technique and Dosimetry: Aapm Report No. 23Subhas SubhasNo ratings yet
- Politi Et Al. - 2015 - Integrated Cooling-Vacuum-Assisted 1540-nm ErGlass Laser Is Effective in Treating Mild-To-Moderate AcneDocument5 pagesPoliti Et Al. - 2015 - Integrated Cooling-Vacuum-Assisted 1540-nm ErGlass Laser Is Effective in Treating Mild-To-Moderate AcneNicolás FarkasNo ratings yet
- Class IV Laser Therapy The Hot Technology of 2011Document3 pagesClass IV Laser Therapy The Hot Technology of 2011JAYAKRISHNANPRNo ratings yet
- Low Level Laser Therapy LLLTDocument9 pagesLow Level Laser Therapy LLLTalamNo ratings yet
- How To Reduce The Fluoroscopy Exposure During TRI Procedure: Li Yue, M.DDocument43 pagesHow To Reduce The Fluoroscopy Exposure During TRI Procedure: Li Yue, M.DmedskyqqNo ratings yet
- Dxa ShieldingDocument21 pagesDxa ShieldingGeorgiana KokonaNo ratings yet
- Radiography Safety ProcedureDocument9 pagesRadiography Safety ProcedureأحمدآلزهوNo ratings yet
- Bilateral CA ToungeDocument5 pagesBilateral CA ToungeDrBadrinarayan SharmaNo ratings yet
- Pigeon Bubble Cpap DeviceDocument2 pagesPigeon Bubble Cpap Deviceteguh nugrohoNo ratings yet
- Edge 4030 Press ReleaseDocument1 pageEdge 4030 Press Releaseapi-432243790No ratings yet
- 11 ADocument5 pages11 AJrar YapNo ratings yet
- 15 Advance TrialDocument35 pages15 Advance TrialShaheen UsmaniNo ratings yet
- Synthon BrochureDocument17 pagesSynthon BrochureTiago MouzinhoNo ratings yet
- Benign Tumors of The StomachDocument55 pagesBenign Tumors of The Stomachapi-19641337No ratings yet
- Amazing Water TherapyDocument4 pagesAmazing Water Therapymil4330No ratings yet
- A Guide For Patients and Physicians: The Washington State Medical Marijuana ActDocument4 pagesA Guide For Patients and Physicians: The Washington State Medical Marijuana Actelioom100% (2)
- Oresol Preparation...............Document24 pagesOresol Preparation...............shielamarie06_ramos3821100% (2)
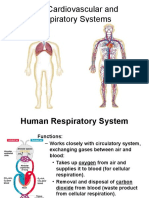
- Cardiovascular and Respiratory SystemDocument51 pagesCardiovascular and Respiratory SystemKarel Mae SanoriaNo ratings yet
- Understanding Clinical Alarm SystemsDocument1 pageUnderstanding Clinical Alarm SystemsPatient Safety MyNo ratings yet
- NMC CBT SAMPLE Q&A PART 3 KEY NURSING CONCEPTSDocument14 pagesNMC CBT SAMPLE Q&A PART 3 KEY NURSING CONCEPTSJoane FranciscoNo ratings yet
- OLFU Intesive Post Test 50 ItemsDocument5 pagesOLFU Intesive Post Test 50 ItemsmonmonNo ratings yet
- How to diagnose autism: Early signs and assessmentsDocument5 pagesHow to diagnose autism: Early signs and assessmentsYeni ZeonNo ratings yet
- Current Status of Health and Disease Burden in IndiaDocument23 pagesCurrent Status of Health and Disease Burden in IndiaKavi rajput100% (1)
- Talon General HospitalDocument22 pagesTalon General HospitalmbalutanNo ratings yet
- Universal Algorithm: Advanced Life SupportDocument1 pageUniversal Algorithm: Advanced Life SupportAndy XiaoNo ratings yet
- Doc-20230413-Wa0000.Document2 pagesDoc-20230413-Wa0000.صادقNo ratings yet
- QR Dengue Infection PDF Final PDFDocument8 pagesQR Dengue Infection PDF Final PDFina2407jrNo ratings yet
- Managing hypertension with bisoprololDocument2 pagesManaging hypertension with bisoprololNovi YulianaNo ratings yet
- DENTAL NETWORK LISTING OF ACCREDITED DENTISTSDocument22 pagesDENTAL NETWORK LISTING OF ACCREDITED DENTISTSRegalado AguhayonNo ratings yet
- Dr. Robert Malone Discusses mRNA Vaccine Platform and COVID LiesDocument13 pagesDr. Robert Malone Discusses mRNA Vaccine Platform and COVID LiesRocco LamponeNo ratings yet
- Applying The Chronic Care Model in Low-Resource Settings Ada Dec2013Document44 pagesApplying The Chronic Care Model in Low-Resource Settings Ada Dec2013Wawan JokoNo ratings yet
- Agnikumara Rasa A Herbo Mineral Formulation ReviewDocument3 pagesAgnikumara Rasa A Herbo Mineral Formulation ReviewEditor IJTSRDNo ratings yet
- PD Case Study: 68yo FemaleDocument9 pagesPD Case Study: 68yo FemaleMary Rose Ponte FernandezNo ratings yet
- Combustio: DR - Dian SyahputraDocument35 pagesCombustio: DR - Dian SyahputraYulliza Kurniawaty LNo ratings yet
- Chronic Groin Pain in An Amateur Soccer Player: Case ReportDocument2 pagesChronic Groin Pain in An Amateur Soccer Player: Case ReportAndreas Arie WidiadiaksaNo ratings yet
- Test Bank For Journey Across The Life Span Human Development and Health Promotion 4th Edition PolanDocument9 pagesTest Bank For Journey Across The Life Span Human Development and Health Promotion 4th Edition PolanGreg RainsNo ratings yet
- Types of DysrhythmiasDocument15 pagesTypes of DysrhythmiasKevin VillaranteNo ratings yet