You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Drug StudyDocument14 pagesDrug Studycruz_johnraymond100% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Philippine College of Physicians Daily Census Ward Hospital de Los Santos-Sti Medical CenterDocument22 pagesPhilippine College of Physicians Daily Census Ward Hospital de Los Santos-Sti Medical Centercruz_johnraymondNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Chapter VIII CDXDocument25 pagesChapter VIII CDXcruz_johnraymondNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Incomplete Abortion Causes and TreatmentDocument3 pagesIncomplete Abortion Causes and Treatmentcruz_johnraymondNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- DEFIBRILLATORDocument3 pagesDEFIBRILLATORcruz_johnraymondNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Book Review QuestionsDocument4 pagesBook Review Questionscruz_johnraymondNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 2ERDocument3 pages2ERcruz_johnraymondNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Case Pres Drugs-CruzDocument7 pagesCase Pres Drugs-Cruzcruz_johnraymondNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Philosophy OF MAN - NumerologyDocument34 pagesPhilosophy OF MAN - Numerologycruz_johnraymond0% (1)
- In Another Country Plot SummeryDocument4 pagesIn Another Country Plot Summerysubto100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Cerebral ContusionDocument88 pagesCerebral ContusionHeaNo ratings yet
- Week#1 AphroditeDocument4 pagesWeek#1 AphroditeFrancisco Javier González GNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- H's and T's of ACLS: A Guide to Differential DiagnosisDocument4 pagesH's and T's of ACLS: A Guide to Differential DiagnosisAnusha Verghese100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Harry Potter Spell ListDocument4 pagesHarry Potter Spell ListEriss RefuerzoNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Adial Orearm Lap: Tor ChiuDocument5 pagesAdial Orearm Lap: Tor ChiuAlNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Netball RulesDocument24 pagesNetball RulesJasmineTeongNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Doberman Pinscher Breed StandardsDocument4 pagesDoberman Pinscher Breed StandardsMorgan Rai LoweNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- MUHS - BPT - 2016 - 4 - Summer - B.P.TH - 51411 Musculoskeletal PhysiotherapyDocument2 pagesMUHS - BPT - 2016 - 4 - Summer - B.P.TH - 51411 Musculoskeletal PhysiotherapyYuvraj AtholeNo ratings yet
- Instruction Manual Guide D'Utilisation Manual de InstruccionesDocument68 pagesInstruction Manual Guide D'Utilisation Manual de InstruccioneslanzeaNo ratings yet
- TCM Patterns Explained: Toxic Heat, Phlegm, Stasis, DeficiencyDocument14 pagesTCM Patterns Explained: Toxic Heat, Phlegm, Stasis, DeficiencyCarleta Stan100% (1)
- CVA620Document80 pagesCVA620Emi DNo ratings yet
- Anatomy II LabDocument48 pagesAnatomy II LabAddicted Outaku اوتاكوNo ratings yet
- Spanish SquatDocument7 pagesSpanish Squatapi-551757456No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Mandibular Nerve BlocksDocument4 pagesMandibular Nerve BlocksNafyiza BaNo ratings yet
- HIRA Fabrication WorkshopDocument316 pagesHIRA Fabrication WorkshopChethan100% (1)
- Snapping Knee Caused by The Gracilis Tendon: A Case Report With An Anatomical StudyDocument5 pagesSnapping Knee Caused by The Gracilis Tendon: A Case Report With An Anatomical StudyDavid BertossiNo ratings yet
- Niel - Camorongan - Project Proposal - First AidawarenessDocument2 pagesNiel - Camorongan - Project Proposal - First AidawarenessJuvielyn JuanNo ratings yet
- ABC TraumaDocument27 pagesABC TraumarikarzNo ratings yet
- Weatherby Vanguard Bolt Action RifleDocument22 pagesWeatherby Vanguard Bolt Action RifleJon MorenoNo ratings yet
- Club Foot CtevDocument82 pagesClub Foot CtevtuyulgaulNo ratings yet
- Magee 6th Edition - OPA - Table of ContentsDocument4 pagesMagee 6th Edition - OPA - Table of ContentsRonny Araya AbarcaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Multi-Specialty Trauma Management GuideDocument163 pagesMulti-Specialty Trauma Management Guideizwan taufikNo ratings yet
- Liston's forgotten splintDocument4 pagesListon's forgotten splintPriyank GuptaNo ratings yet
- Étude Du Centre de Traitement Des Lésions Cérébrales de L'université de DalhousieDocument41 pagesÉtude Du Centre de Traitement Des Lésions Cérébrales de L'université de DalhousieRadio-Canada100% (2)
- Ling Wu Case NotesDocument3 pagesLing Wu Case NotesOana Maria Grigore77% (13)
- Trestles and StagingDocument2 pagesTrestles and Stagingdak comeiNo ratings yet
- Posterior Tibialis Tendonitis StudyDocument6 pagesPosterior Tibialis Tendonitis StudyShane WetzelNo ratings yet
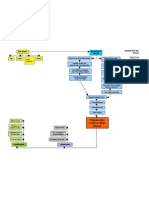
- Degenerative Disc Disease Concept MapDocument1 pageDegenerative Disc Disease Concept MapashleydeanNo ratings yet
- Meniscus TearsDocument29 pagesMeniscus Tearsmaulana ilhamNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)