You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Norma Japonesa Aij-Rlb-1996Document36 pagesNorma Japonesa Aij-Rlb-1996AnaApcarianNo ratings yet
- Wiki Unified Soil Classification SystemDocument2 pagesWiki Unified Soil Classification SystemGIRISHA001No ratings yet
- Instructivo Luxometro Steren Her-410 PDFDocument12 pagesInstructivo Luxometro Steren Her-410 PDFLuis CárdenasNo ratings yet
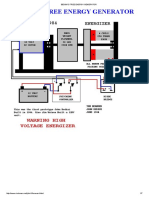
- Bedini's Free Energy Generator PDFDocument7 pagesBedini's Free Energy Generator PDFRafly Attila Al-Fiqri71% (7)
- Elders Ray SYstemsDocument7 pagesElders Ray SYstemssagarmkale4395No ratings yet
- Bearings ShaftsDocument74 pagesBearings ShaftsCik MinnNo ratings yet
- CH 10 Circular Motion Exercises AnswersDocument4 pagesCH 10 Circular Motion Exercises AnswersMuhammad Aslam0% (1)
- Cementing EquipDocument12 pagesCementing Equipzbhdzp100% (1)
- Cati Pakistan Training Course - MechanicalDocument13 pagesCati Pakistan Training Course - MechanicalImam Haryadi WibowoNo ratings yet
- Gay-Lussac's Law Problems and SolutionsDocument1 pageGay-Lussac's Law Problems and SolutionsBasic PhysicsNo ratings yet
- 08 Energy 03 Complementary Strain Energy PDFDocument2 pages08 Energy 03 Complementary Strain Energy PDFjack_hero_56No ratings yet
- Interference PatternsDocument8 pagesInterference PatternsAsa mathewNo ratings yet
- Anti Derivative Chain RuleDocument4 pagesAnti Derivative Chain Ruletutorciecle123No ratings yet
- Bleeding of ConcreteDocument3 pagesBleeding of ConcreteANo ratings yet
- Solution Manual-Chemical Engineering Thermodynamics - Smith Van NessDocument621 pagesSolution Manual-Chemical Engineering Thermodynamics - Smith Van NessSurya Budi Widagdo87% (184)
- CH20005-Chemical Reaction Engineering:) C C CRDocument2 pagesCH20005-Chemical Reaction Engineering:) C C CRSunny KashyapNo ratings yet
- L-3/T-2/CE Date: 07/08/2016Document30 pagesL-3/T-2/CE Date: 07/08/2016নীল জোছনা0% (1)
- MCQ Electromagnetism Self-AssessmentDocument2 pagesMCQ Electromagnetism Self-AssessmentJunaidKhanNo ratings yet
- Numerical Programming I (For CSE) : Final ExamDocument7 pagesNumerical Programming I (For CSE) : Final ExamhisuinNo ratings yet
- Harmonic Oscillator & Rigid Rotor ModelsDocument14 pagesHarmonic Oscillator & Rigid Rotor ModelsJisu RyuNo ratings yet
- Homework #02 (Phy 112) SolutionsDocument19 pagesHomework #02 (Phy 112) SolutionsKvn4N6No ratings yet
- Beryllium and Beryllium Compounds: 2005 Wiley-Vch Verlag GMBH & Co. Kgaa, WeinheimDocument28 pagesBeryllium and Beryllium Compounds: 2005 Wiley-Vch Verlag GMBH & Co. Kgaa, WeinheimjaimeNo ratings yet
- The Optical ProThe Optical Properties of Lung As A Function of Respirationperties of Lung As A Function ofDocument11 pagesThe Optical ProThe Optical Properties of Lung As A Function of Respirationperties of Lung As A Function ofAgustinNo ratings yet
- Refractive Index of A Liquid (Theory) : Class 12: PhysicsDocument4 pagesRefractive Index of A Liquid (Theory) : Class 12: PhysicsAmartya AnshumanNo ratings yet
- EssayDocument5 pagesEssayRobert MariasiNo ratings yet
- Relationships and Lattices in AlgebraDocument2 pagesRelationships and Lattices in AlgebraRadhika RathoreNo ratings yet
- BelowsDocument35 pagesBelowstejassidhpuraNo ratings yet
- Chapter - 3.2 - Finale Internal Forced ConvectionDocument18 pagesChapter - 3.2 - Finale Internal Forced ConvectioneirinaNo ratings yet
- 960 Physics (PPU) Semester 2 Topics-SyllabusDocument7 pages960 Physics (PPU) Semester 2 Topics-SyllabusJosh, LRT0% (1)
- Teacher Guide Activity 2 AccelerationDocument4 pagesTeacher Guide Activity 2 AccelerationCanada Railway TimesNo ratings yet