You might also like
- Understanding Brain Tumors in 40 CharactersDocument46 pagesUnderstanding Brain Tumors in 40 CharactersJoyce Minerva Montero SamsonNo ratings yet
- Brain CancerDocument33 pagesBrain Cancermynoidanh19No ratings yet
- Brain TumorDocument67 pagesBrain TumorNur AgamiNo ratings yet
- Types of CancerDocument7 pagesTypes of CancerRegina SABSNo ratings yet
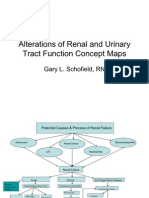
- Renal Concept MapDocument8 pagesRenal Concept MapRob DavilaNo ratings yet
- Burn Injury PathophysiologyDocument1 pageBurn Injury PathophysiologyMonique Ann DanoyNo ratings yet
- Polymyositis and Dermatomyositis: Symptoms, Signs, Diagnosis and TreatmentDocument5 pagesPolymyositis and Dermatomyositis: Symptoms, Signs, Diagnosis and Treatmentdeea03No ratings yet
- Aging Brain Changes May Cause Inappropriate Social BehaviorDocument5 pagesAging Brain Changes May Cause Inappropriate Social BehaviorBorlongan PaulineNo ratings yet
- Chronic Lymphocytic LeukemiaDocument6 pagesChronic Lymphocytic LeukemiaJhannNo ratings yet
- The Genetic Basis of CancerDocument31 pagesThe Genetic Basis of Cancerapi-418176886No ratings yet
- Pathology Case Presentation: Prepared by Roll No.s 1-9Document20 pagesPathology Case Presentation: Prepared by Roll No.s 1-9vishalzenia100% (1)
- The Way of The ShepherdDocument6 pagesThe Way of The ShepherdAnj De GuzmanNo ratings yet
- Jurnal - EuthanasiaDocument8 pagesJurnal - EuthanasiaMacenNo ratings yet
- Pathology of Thyroid DiseasesDocument5 pagesPathology of Thyroid DiseasesNur Kamalia KamalNo ratings yet
- Acute Myeloid Leukemia (Drug Study)Document3 pagesAcute Myeloid Leukemia (Drug Study)Krisianne Mae Lorenzo FranciscoNo ratings yet
- Disorders of The Thyroid GlandDocument21 pagesDisorders of The Thyroid GlandAgustina TambingNo ratings yet
- Oncology Nursing - OverviewDocument137 pagesOncology Nursing - OverviewMae DacerNo ratings yet
- Carcinoma of The Breast - Bailey & LoveDocument5 pagesCarcinoma of The Breast - Bailey & LoveKeyshia Yazid100% (1)
- Agis Mira Dewi, S.kedDocument35 pagesAgis Mira Dewi, S.kedAgiish EMdeNo ratings yet
- Epidemiology, Pathology, Clinical Features, and Diagnosis of Meningioma - UpToDateDocument22 pagesEpidemiology, Pathology, Clinical Features, and Diagnosis of Meningioma - UpToDatewilson kores100% (1)
- Oncology Nursing-2 PDFDocument22 pagesOncology Nursing-2 PDFHebsiba PonnayyanNo ratings yet
- Bladder CancerDocument39 pagesBladder CancerAlfred BantigueNo ratings yet
- Phosphate Imbalances PDFDocument1 pagePhosphate Imbalances PDFKaye RicoNo ratings yet
- Concept Map InstructionsDocument2 pagesConcept Map InstructionsKatherine Conlu BenganNo ratings yet
- Ovarian Cancer AlvezaDocument13 pagesOvarian Cancer AlvezaYa Mei Li100% (1)
- Cancer Case StudyDocument33 pagesCancer Case StudyBorlongan PaulineNo ratings yet
- Prayer Before the EucharistDocument115 pagesPrayer Before the EucharistMicah RamaykaNo ratings yet
- 1.2 Purpose of Cystoclysis: 1. Closed Bladder Irrigation SystemDocument6 pages1.2 Purpose of Cystoclysis: 1. Closed Bladder Irrigation SystemKatleen Calang AlagNo ratings yet
- Gastric CarcinomaDocument21 pagesGastric CarcinomaAli Abbas100% (2)
- GBS Nursing MangementDocument21 pagesGBS Nursing MangementJoseph Namita SunnyNo ratings yet
- Chemotherapy and Biotherapy Hypersensitivity Reactions: Christine E. Coyle, RN, BSN, OCNDocument55 pagesChemotherapy and Biotherapy Hypersensitivity Reactions: Christine E. Coyle, RN, BSN, OCNRakesh MishraNo ratings yet
- GiardiaDocument14 pagesGiardiaA Gabitza LuNo ratings yet
- Brain TumorDocument50 pagesBrain TumorbudiNo ratings yet
- Testicular CancerDocument48 pagesTesticular Cancerluckyswiss7776848No ratings yet
- Reflective Essay Guide.Document4 pagesReflective Essay Guide.Aldana RodríguezNo ratings yet
- My management philosophy is guiding employeesDocument2 pagesMy management philosophy is guiding employeesLeur Morata Sazreuf100% (1)
- Prostate Cancer: Symptoms, Diagnosis, Treatment, and RehabilitationDocument4 pagesProstate Cancer: Symptoms, Diagnosis, Treatment, and RehabilitationParixit DasNo ratings yet
- Bacterial Pneumonia PharmacologyDocument70 pagesBacterial Pneumonia PharmacologyMarc Imhotep Cray, M.D.No ratings yet
- Systemic Lupus ErythematosusDocument5 pagesSystemic Lupus ErythematosusVane UcatNo ratings yet
- FractureDocument302 pagesFractureMaryjoy Gabriellee De La CruzNo ratings yet
- How Does Radiation Therapy Work?Document5 pagesHow Does Radiation Therapy Work?mikeadrianNo ratings yet
- Hysterectomy and Bilateral Salpingo-OophorectomyDocument1 pageHysterectomy and Bilateral Salpingo-Oophorectomyapi-3712326100% (3)
- Acute Abdomen The "Black Hole" of MedicineDocument99 pagesAcute Abdomen The "Black Hole" of MedicinedebarajuNo ratings yet
- Renal Cell CarcinomaDocument15 pagesRenal Cell Carcinomadger11No ratings yet
- JhelaiDocument1 pageJhelaiWinjel AnnNo ratings yet
- DR Tommy - Cancer PainDocument60 pagesDR Tommy - Cancer PainrisalbaluNo ratings yet
- NU602 Unit 2 Assignment Patricia BennerDocument23 pagesNU602 Unit 2 Assignment Patricia BennerPaulRoppFLNo ratings yet
- Adjuvant breast cancer therapy agentsDocument3 pagesAdjuvant breast cancer therapy agentsGem BulaongNo ratings yet
- Adrenal Gland Disorders ExplainedDocument48 pagesAdrenal Gland Disorders ExplainedMubeenUrRehmanNo ratings yet
- Idiopathic Thrombocytopenic PurpuraDocument45 pagesIdiopathic Thrombocytopenic PurpuraOhnesan Medina PerezNo ratings yet
- Managing Psychiatric Patients in The EDDocument28 pagesManaging Psychiatric Patients in The EDfadiNo ratings yet
- Dengue FeverDocument5 pagesDengue FeverMae AzoresNo ratings yet
- The Challenges of Offshoring and Outsourcing.Document7 pagesThe Challenges of Offshoring and Outsourcing.Bopzilla0911No ratings yet
- ShockDocument21 pagesShockMin-Joo Esther ParkNo ratings yet
- This Study Resource Was Shared Via: HypoparathyroidismDocument1 pageThis Study Resource Was Shared Via: HypoparathyroidismDeo FactuarNo ratings yet
- Acute Lymphocytic LeukemiaDocument7 pagesAcute Lymphocytic LeukemiaKim Enrico JumarangNo ratings yet
- Physiological Effect of AgingDocument4 pagesPhysiological Effect of AgingSandra MeruNo ratings yet
- Case Study FinalDocument77 pagesCase Study FinalMacey Malonzo100% (1)
- Brain Tumour GuideDocument11 pagesBrain Tumour GuidesonyNo ratings yet
- Brain Tumor Increased Icp Head Neck Ca and Tracheostomy VillamorDocument24 pagesBrain Tumor Increased Icp Head Neck Ca and Tracheostomy Villamorchristian pulmonesNo ratings yet
- CC Boot GameDocument18 pagesCC Boot GamePapz DockieNo ratings yet
- Esophageal CADocument25 pagesEsophageal CADan Kenneth83% (6)
- Prostate CancerDocument31 pagesProstate CancerDan KennethNo ratings yet
- Nurses PrayerDocument1 pageNurses PrayerDan KennethNo ratings yet
- Nursing Management in Cancer CareDocument71 pagesNursing Management in Cancer CareDan KennethNo ratings yet
- C Yyyyyyyyy Yyyy YyDocument30 pagesC Yyyyyyyyy Yyyy YyDan KennethNo ratings yet
- Ankle SprainDocument3 pagesAnkle SprainDan KennethNo ratings yet
- ReadingsDocument10 pagesReadingsDan KennethNo ratings yet
- C Yyyyyyyyy Yyyy YyDocument30 pagesC Yyyyyyyyy Yyyy YyDan KennethNo ratings yet
- The Nervous SystemDocument53 pagesThe Nervous SystemDan KennethNo ratings yet
- Your Ultimate BrainDocument3 pagesYour Ultimate BrainwinashijNo ratings yet
- Chapter 1-5Document181 pagesChapter 1-5tolera bedadaNo ratings yet
- Brain Mapping An Encyclopedic Reference (-PUNISHER-)Document2,668 pagesBrain Mapping An Encyclopedic Reference (-PUNISHER-)Robin Smith100% (5)
- Science: Quarter 2 - Module 3: From Cell To OrganismDocument17 pagesScience: Quarter 2 - Module 3: From Cell To OrganismMelody SorianoNo ratings yet
- Kuis Modul 1.2 1Document5 pagesKuis Modul 1.2 1Wijoyo KusumoNo ratings yet
- Anatomy Physiology of Human BodyDocument90 pagesAnatomy Physiology of Human BodyJesica ElviraNo ratings yet
- Anastasia Novykh Spiritual Practices and MeditationsDocument134 pagesAnastasia Novykh Spiritual Practices and MeditationsHadronski Kolajder100% (2)
- Physiology - Nervous System - MCQDocument13 pagesPhysiology - Nervous System - MCQadham100% (1)
- Fraser - Time and Time Again-Reports From A Boundary of The Universe - 900415485XDocument448 pagesFraser - Time and Time Again-Reports From A Boundary of The Universe - 900415485XTofan Alin100% (2)
- Annals of Behavioral Neuroscience Research Article: ISSN: 2638-9231Document29 pagesAnnals of Behavioral Neuroscience Research Article: ISSN: 2638-9231navinavinaviNo ratings yet
- Lateralidad y Orietacion Espacial, Niños Con Dislexia PDFDocument8 pagesLateralidad y Orietacion Espacial, Niños Con Dislexia PDFCa LúNo ratings yet
- PSYU1101 - Essay IDocument7 pagesPSYU1101 - Essay IaangieeNo ratings yet
- IPP Ted Listening SeriesDocument226 pagesIPP Ted Listening SeriesNhungNo ratings yet
- OBT Draft PersonalityDocument8 pagesOBT Draft PersonalityMuskan KaurNo ratings yet
- Psychology Themes and Variations Canadian 4th Edition Weiten Test BankDocument39 pagesPsychology Themes and Variations Canadian 4th Edition Weiten Test Bankleowright2n3k100% (11)
- The Power of Neuro-PlasticityDocument31 pagesThe Power of Neuro-PlasticityNing JiaNo ratings yet
- Fall 2022 - ZOO403 - 1 - BC190408115Document4 pagesFall 2022 - ZOO403 - 1 - BC190408115Misbah NoreenNo ratings yet
- Allport 1985 Distributed Memory Modular Subsystems and Dysphasia PDFDocument15 pagesAllport 1985 Distributed Memory Modular Subsystems and Dysphasia PDFavastudioNo ratings yet
- 7 AttentionDocument16 pages7 AttentionZidane ZizouNo ratings yet
- Auspicium NLP Practitioner QuestionsDocument21 pagesAuspicium NLP Practitioner QuestionsashishsipaiNo ratings yet
- Adult Total Body Detox GuideDocument40 pagesAdult Total Body Detox GuideemanvitoriaNo ratings yet
- Avatar - Project Aims For Human Immortality by 2045Document8 pagesAvatar - Project Aims For Human Immortality by 2045Mel DsaNo ratings yet
- Full Download Test Bank For Health Psychology 3rd Canadian Edition PDF Full ChapterDocument36 pagesFull Download Test Bank For Health Psychology 3rd Canadian Edition PDF Full Chapterrequinneologic8yzqgt100% (17)
- Biological Basis of Learning and MemoryDocument30 pagesBiological Basis of Learning and MemoryParamesh WaranNo ratings yet
- Eth 102LDocument6 pagesEth 102LAnonymous 188AFiNo ratings yet
- Cognitive NeuroscienceDocument526 pagesCognitive NeuroscienceVelimir Topolovec90% (21)
- Environmental Enrichment As A Therapy For Autism - A Clinical Trial Replication and Extension PDFDocument11 pagesEnvironmental Enrichment As A Therapy For Autism - A Clinical Trial Replication and Extension PDFJoan RodríguezNo ratings yet
- Study Guide Lin 2601Document192 pagesStudy Guide Lin 2601Joanne100% (1)
- Tsa International Sample PaperDocument36 pagesTsa International Sample PaperEila AbdullahNo ratings yet
- Test Bank For Seeleys Anatomy Physiology 12th by VanputteDocument36 pagesTest Bank For Seeleys Anatomy Physiology 12th by Vanputteunco.forcut.rlln100% (41)