You might also like
- Undescended Testis: DR - Santosh Jha TMUDocument33 pagesUndescended Testis: DR - Santosh Jha TMUYamir Fernando Monroy MartínNo ratings yet
- Undescended TestesDocument29 pagesUndescended TestesHillary Bushnell100% (1)
- CERVICAL LYMPADENOPATHY - EduardDocument34 pagesCERVICAL LYMPADENOPATHY - EduardYemima Divinadia100% (1)
- Open Fracture - GustiloDocument9 pagesOpen Fracture - GustiloWan Hafiz W YusoffNo ratings yet
- Congenital Malformations of The Female Genital TractDocument7 pagesCongenital Malformations of The Female Genital TractDo le QuangNo ratings yet
- GYNE 4.01a EndometriosisDocument4 pagesGYNE 4.01a EndometriosisGray SnellNo ratings yet
- Phyllodes TumorDocument20 pagesPhyllodes TumorManuela KarinaaNo ratings yet
- Benign Anorectal Conditions: Ahmed Badrek-AmoudiDocument20 pagesBenign Anorectal Conditions: Ahmed Badrek-AmoudiAna De La RosaNo ratings yet
- EndometriosisDocument7 pagesEndometriosisIsabel CastilloNo ratings yet
- Examination of Breast Lump PDFDocument2 pagesExamination of Breast Lump PDFDanaNo ratings yet
- Necrotizing EnterocolitisDocument36 pagesNecrotizing EnterocolitisMahad Maxamed AxmedNo ratings yet
- Diseases of The Female Genital TractDocument4 pagesDiseases of The Female Genital Tractsarguss14No ratings yet
- Endometrial Hyperplasia: by Dr. Mervat AliDocument48 pagesEndometrial Hyperplasia: by Dr. Mervat AliAsh AmeNo ratings yet
- GYNE 4.01b InfertilityDocument4 pagesGYNE 4.01b InfertilityGray SnellNo ratings yet
- Hematuria in ChildrenDocument26 pagesHematuria in ChildrenNovenZefanya100% (1)
- Premalignant Lesions of The CervixDocument22 pagesPremalignant Lesions of The Cervixkaren carpioNo ratings yet
- Pediatric Surgery Dr. A. IgamaDocument6 pagesPediatric Surgery Dr. A. IgamaMarco Paulo Reyes NaoeNo ratings yet
- GYNE 4.05a Bening Ang Malignant Lesions of The VulvaDocument11 pagesGYNE 4.05a Bening Ang Malignant Lesions of The VulvaGray SnellNo ratings yet
- Pathology of TestesDocument4 pagesPathology of TestesGerardLum100% (1)
- Perforated Gastric UlcerDocument18 pagesPerforated Gastric UlcerNorshahidah IedaNo ratings yet
- Urinary IncontinenceDocument1 pageUrinary IncontinenceZiyad100% (1)
- Medicine 6.1b Approach To Cancer Patients - FernandoDocument7 pagesMedicine 6.1b Approach To Cancer Patients - FernandoAbigail LausNo ratings yet
- GYNE 4.06-Benign and Malignant Lesions of UterusDocument7 pagesGYNE 4.06-Benign and Malignant Lesions of UterusGray SnellNo ratings yet
- Abdominal Wound Dehiscence: DR - Nazmoon Nahar Honorary Medical Officer Surgery Unit IIIDocument18 pagesAbdominal Wound Dehiscence: DR - Nazmoon Nahar Honorary Medical Officer Surgery Unit IIIMashrufNo ratings yet
- Dr. Sharda Jain: Director: Secretary GeneralDocument91 pagesDr. Sharda Jain: Director: Secretary GeneraljijaniNo ratings yet
- Urethral Stricture DiseaseDocument9 pagesUrethral Stricture DiseaseIntanAgustiFernandesNo ratings yet
- MPNST Diagnosis and TreatmentDocument27 pagesMPNST Diagnosis and TreatmentrahadiyantiNo ratings yet
- EAU Guidelines Urolithiasis 2016Document82 pagesEAU Guidelines Urolithiasis 2016andrilulusanterbaikNo ratings yet
- Pathology 5.05b Vagina and Vulva - DR - Dy (Final Edit)Document11 pagesPathology 5.05b Vagina and Vulva - DR - Dy (Final Edit)Dranreb Berylle MasangkayNo ratings yet
- EmpyemaDocument17 pagesEmpyemaNoviaCandraDwipaNo ratings yet
- Penetrating Abdominal Injury DiagnosisDocument3 pagesPenetrating Abdominal Injury DiagnosisRaquel ReyesNo ratings yet
- Henoch Schonlein Purpura REVDocument42 pagesHenoch Schonlein Purpura REVBayu Kurniawan100% (1)
- Patogenesis Infeksi BakteriDocument47 pagesPatogenesis Infeksi BakteribellabelbonNo ratings yet
- CardiotocographyDocument27 pagesCardiotocographyJesica CahyadyNo ratings yet
- Albendazole in PediatricsDocument38 pagesAlbendazole in PediatricsKishore ChandkiNo ratings yet
- Compartment Syndrome: Sebelas Maret UniversityDocument8 pagesCompartment Syndrome: Sebelas Maret Universitykhrisna satyaksaNo ratings yet
- Uterine FibroidsDocument21 pagesUterine FibroidsPrasun BiswasNo ratings yet
- Gyne - Case 15 Benign Lesions of The Vulva & VaginaDocument2 pagesGyne - Case 15 Benign Lesions of The Vulva & Vaginacbac1990No ratings yet
- Varicose Vein FinalDocument60 pagesVaricose Vein FinalblitheleevsNo ratings yet
- Pediatric Surgery EmergencyDocument48 pagesPediatric Surgery EmergencyputraNo ratings yet
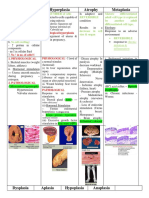
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument20 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- Appendectomy GuidelinesDocument12 pagesAppendectomy GuidelinesJessa Frances FranciscoNo ratings yet
- Pathogens of The Female Reproductive System - Leah NechamkinDocument1 pagePathogens of The Female Reproductive System - Leah NechamkinMicroposterNo ratings yet
- Clinic-Pharmacologic Approaches To Antimicrobial Therapy in Surgical InfectionsDocument27 pagesClinic-Pharmacologic Approaches To Antimicrobial Therapy in Surgical InfectionsMuhammad NaveedNo ratings yet
- Dr. Kunta Setiaji (ThyroidNodule)Document17 pagesDr. Kunta Setiaji (ThyroidNodule)Hasty WahyuniNo ratings yet
- Pediatric Tuberculosis: Causes, Symptoms and TreatmentDocument112 pagesPediatric Tuberculosis: Causes, Symptoms and TreatmentFenny RahmadaniNo ratings yet
- Pyloric Stenosis Guide: Causes, Symptoms, DiagnosisDocument23 pagesPyloric Stenosis Guide: Causes, Symptoms, DiagnosisRama ItachiNo ratings yet
- Hernia: and Other Digestive Congenital DiseaseDocument14 pagesHernia: and Other Digestive Congenital DiseaseLingga GumelarNo ratings yet
- Benign Gynecological LesionsDocument9 pagesBenign Gynecological LesionsLanceNo ratings yet
- Pelvic FracturesDocument8 pagesPelvic FracturesArif AbubakarNo ratings yet
- Scabies RijiDocument29 pagesScabies RijirijivincentNo ratings yet
- Surgery ParathyroidDocument11 pagesSurgery ParathyroidMATTHEW EARL MALUMAYNo ratings yet
- Safe and Optimum Steps For Total / Hemi Thyroidectomy: Otolaryngology Open Access JournalDocument4 pagesSafe and Optimum Steps For Total / Hemi Thyroidectomy: Otolaryngology Open Access JournalJerahmeel Sombilon GenillaNo ratings yet
- Acute Abdomen: - DefinitionDocument27 pagesAcute Abdomen: - DefinitionWorku KifleNo ratings yet
- Anaemia in Pregnancy md3 MhsDocument26 pagesAnaemia in Pregnancy md3 MhsjerrydanfordfxNo ratings yet
- Hirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshDocument48 pagesHirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshArchana Mahata100% (1)
- Intrauterine Fetal Demise (IUFD)Document4 pagesIntrauterine Fetal Demise (IUFD)skrameer100% (1)
- Acute AbdomenDocument2 pagesAcute AbdomenTroy FengNo ratings yet
- Urology 36 Undescended TestisDocument33 pagesUrology 36 Undescended TestistasyaNo ratings yet
- Urology 36 Undescended TestisDocument33 pagesUrology 36 Undescended TestistasyaNo ratings yet
- 6 BwahDocument6 pages6 BwahMartha PNo ratings yet
- STDDocument72 pagesSTDMartha PNo ratings yet
- Sexually Transmitted DiseaseDocument39 pagesSexually Transmitted DiseaseMartha PNo ratings yet
- Sexually Transmitted Diseases (STD'S)Document40 pagesSexually Transmitted Diseases (STD'S)Martha P100% (1)
- BancroftDocument23 pagesBancroftMartha PNo ratings yet
- Sexually Transmitted Diseases A.K.A Sexually Transmitted InfectionsDocument20 pagesSexually Transmitted Diseases A.K.A Sexually Transmitted InfectionsMartha PNo ratings yet
- Sexually Transmitted DiseasesDocument14 pagesSexually Transmitted DiseasesMartha P0% (1)
- Bay KuniDocument10 pagesBay KuniMartha PNo ratings yet
- Hypospadias Surgery TechniquesDocument45 pagesHypospadias Surgery TechniquesMartha P100% (1)
- Journal PsikiatriDocument7 pagesJournal PsikiatriUva TwittNo ratings yet
- Norah JonesDocument2 pagesNorah JonesMartha PNo ratings yet
- Uas SoslitDocument9 pagesUas SoslitMartha PNo ratings yet
- Table of ContentsDocument2 pagesTable of Contentsulum21No ratings yet
- Recent Developments in Carbapenems: ReviewDocument16 pagesRecent Developments in Carbapenems: ReviewFrancielleNo ratings yet
- Transactional Analysis (TA)Document21 pagesTransactional Analysis (TA)Rohan TandonNo ratings yet
- Sister Letty G. Kuan Retirement and Role DiscontinuitiesDocument26 pagesSister Letty G. Kuan Retirement and Role DiscontinuitiesAbigail Faith Pretesto100% (1)
- Final Draft - Banana ChipsDocument34 pagesFinal Draft - Banana ChipsAubrey Delgado74% (35)
- Phychem Expt. 1Document8 pagesPhychem Expt. 1Bren Julius PabloNo ratings yet
- ITC's diverse businesses: cigarettes, packaging, hotels, paperboards, stationery, matches, incense sticks, retail, food, exportsDocument1 pageITC's diverse businesses: cigarettes, packaging, hotels, paperboards, stationery, matches, incense sticks, retail, food, exportsShashank JainNo ratings yet
- Firemac FM Fire Ducts Provide Fire Resistant VentilationDocument12 pagesFiremac FM Fire Ducts Provide Fire Resistant Ventilationsiva8784No ratings yet
- Tan Trok Tam Devi Suk TamDocument4 pagesTan Trok Tam Devi Suk Tamtejasg82No ratings yet
- Full Test 14 (Key) PDFDocument4 pagesFull Test 14 (Key) PDFhoang lichNo ratings yet
- Lecture 4 Part 1 PDFDocument11 pagesLecture 4 Part 1 PDFBashar AntriNo ratings yet
- 1 s2.0 S0149763418301957 MainDocument24 pages1 s2.0 S0149763418301957 MainjackNo ratings yet
- Pnp-MemorandumDocument9 pagesPnp-MemorandumraalphNo ratings yet
- Manufacturing ProcessDocument6 pagesManufacturing Processbro nawalibmatNo ratings yet
- Communicating Across AgesDocument35 pagesCommunicating Across AgesConrad TarihoranNo ratings yet
- JMPR 2010 ContentsDocument55 pagesJMPR 2010 ContentsTÙNGNo ratings yet
- EPG Health Report The Future of HCP Engagement Impact 2023Document73 pagesEPG Health Report The Future of HCP Engagement Impact 2023paulilongereNo ratings yet
- Handout2 Fischer CarbeneDocument5 pagesHandout2 Fischer CarbeneMuhammad ShimaNo ratings yet
- Prof. J.L. HumarOffice: HP 3051Phone: 613-520-2600 ext. 3051Email: jhumar@cmail.carleton.caOffice Hours: Tuesdays and Thursdays, 2:00-3:00 pmDocument2 pagesProf. J.L. HumarOffice: HP 3051Phone: 613-520-2600 ext. 3051Email: jhumar@cmail.carleton.caOffice Hours: Tuesdays and Thursdays, 2:00-3:00 pmBhind NijjarNo ratings yet
- Climate and Cultural IdentityDocument2 pagesClimate and Cultural IdentityCha AbolucionNo ratings yet
- ThesisDocument26 pagesThesiscmomcqueenNo ratings yet
- Chapter Test A: Teacher Notes and Answers 17Document5 pagesChapter Test A: Teacher Notes and Answers 17Mmf 123 JanNo ratings yet
- Calcul BADocument15 pagesCalcul BAHanane BenGamraNo ratings yet
- A Lesson Design in HELE 6 Chapter 2Document6 pagesA Lesson Design in HELE 6 Chapter 2Jestoni Paragsa100% (5)
- Unit 23 The Interior LandscapeDocument21 pagesUnit 23 The Interior LandscapesNo ratings yet
- 5 Ethiopian - National - Healthcare - Quality - and - Safety - Strategy - Final - Draft-July122021Document86 pages5 Ethiopian - National - Healthcare - Quality - and - Safety - Strategy - Final - Draft-July122021Kemal MahmoudNo ratings yet
- Wildseed Dinner MenuDocument1 pageWildseed Dinner MenuCaleb PershanNo ratings yet
- Mms For Household Uses-S.pardee-1Document7 pagesMms For Household Uses-S.pardee-1Manny JorgeNo ratings yet
- Bangladesh National Building Code 2012 Part 07 - Construction Practices and SafetyDocument83 pagesBangladesh National Building Code 2012 Part 07 - Construction Practices and SafetyPranoy Barua100% (3)
- StarFish BrochureDocument9 pagesStarFish BrochureSaepul HerdianNo ratings yet
- 20K-S100 - CK20S10 - 21MK50-Chasis SN-80 SharpDocument26 pages20K-S100 - CK20S10 - 21MK50-Chasis SN-80 SharpAmadou FallNo ratings yet