You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- UWorld Notes Step 2 CKDocument11 pagesUWorld Notes Step 2 CKSamah Khan50% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Pathophysiology of BurnDocument3 pagesPathophysiology of Burnuaeb100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Investing 101 For Residents: RJ Nemeyer MDDocument12 pagesInvesting 101 For Residents: RJ Nemeyer MDEmily EresumaNo ratings yet
- PQCNC AIM RPC LS2 Volunteer Doula ProgramDocument23 pagesPQCNC AIM RPC LS2 Volunteer Doula ProgramkcochranNo ratings yet
- Morning Report: Lindsey Gakenheimer-Smith MD PGY3Document20 pagesMorning Report: Lindsey Gakenheimer-Smith MD PGY3Emily EresumaNo ratings yet
- Board Prep Emergency Ingestions Dec.2018Document46 pagesBoard Prep Emergency Ingestions Dec.2018Emily EresumaNo ratings yet
- Board Prep Metabolics Feb 2019Document23 pagesBoard Prep Metabolics Feb 2019Emily EresumaNo ratings yet
- Case Study of Ruptured Appendicitis With Localize Peritonitis (Final)Document76 pagesCase Study of Ruptured Appendicitis With Localize Peritonitis (Final)DRJC82% (22)
- Halloween Safety: Dominique ChevalierDocument21 pagesHalloween Safety: Dominique ChevalierEmily EresumaNo ratings yet
- Prevent Coronavirus InfectionDocument16 pagesPrevent Coronavirus InfectionFitri ThreeanNo ratings yet
- Ventilators 11.07.2018Document38 pagesVentilators 11.07.2018Emily EresumaNo ratings yet
- Pediatric Urology Topics Relating To Infants & Toddlers: Danielle Brady, Pgy-2Document35 pagesPediatric Urology Topics Relating To Infants & Toddlers: Danielle Brady, Pgy-2Emily EresumaNo ratings yet
- Lecture 1 History of SurgeryDocument7 pagesLecture 1 History of SurgeryRosa PalconitNo ratings yet
- Morning Report Case Presentation: APRIL 1, 2019Document14 pagesMorning Report Case Presentation: APRIL 1, 2019Emily EresumaNo ratings yet
- Food Challenge 03.20.2019Document17 pagesFood Challenge 03.20.2019Emily EresumaNo ratings yet
- Kidney Disorders 03.27.2019Document33 pagesKidney Disorders 03.27.2019Emily EresumaNo ratings yet
- Ophtho Pearls 03.13.2019Document17 pagesOphtho Pearls 03.13.2019Emily EresumaNo ratings yet
- Dangers of Vaping 03.15.2019Document23 pagesDangers of Vaping 03.15.2019Emily EresumaNo ratings yet
- Pediatric Hypertension Noon Conference 03.20.2019Document44 pagesPediatric Hypertension Noon Conference 03.20.2019Emily EresumaNo ratings yet
- Tachycardia How To Keep Your Patient Alive in The Middle of The NightDocument30 pagesTachycardia How To Keep Your Patient Alive in The Middle of The NightEmily Eresuma100% (1)
- Pertussis 01.14.2019Document29 pagesPertussis 01.14.2019Emily EresumaNo ratings yet
- Case Presentation: Tad MiyaDocument41 pagesCase Presentation: Tad MiyaEmily EresumaNo ratings yet
- Board Prep GI Jan 2019Document32 pagesBoard Prep GI Jan 2019Emily EresumaNo ratings yet
- Somatization 01.28.2019Document28 pagesSomatization 01.28.2019Emily EresumaNo ratings yet
- Bells Palsy or Stroke 02.06.2019Document19 pagesBells Palsy or Stroke 02.06.2019Emily EresumaNo ratings yet
- Board Prep Genetics Dec 2018Document62 pagesBoard Prep Genetics Dec 2018Emily EresumaNo ratings yet
- Chronic Granulomatous Disease 01.23.2019Document10 pagesChronic Granulomatous Disease 01.23.2019Emily EresumaNo ratings yet
- Anemia: Erika Franz-O'Neal PGY-2 Pediatric ResidentDocument16 pagesAnemia: Erika Franz-O'Neal PGY-2 Pediatric ResidentEmily EresumaNo ratings yet
- MysteryCase 10.22.18Document10 pagesMysteryCase 10.22.18Emily EresumaNo ratings yet
- Morning Report: JANUARY 7, 2019 Katie Mailey, Pgy2Document24 pagesMorning Report: JANUARY 7, 2019 Katie Mailey, Pgy2Emily EresumaNo ratings yet
- Morning Report: Melanie Nelson, PGY-2Document25 pagesMorning Report: Melanie Nelson, PGY-2Emily EresumaNo ratings yet
- Morning Report: Wade Harrison, MD, MPHDocument13 pagesMorning Report: Wade Harrison, MD, MPHEmily EresumaNo ratings yet
- Limping 12.10.2018Document32 pagesLimping 12.10.2018Emily Eresuma100% (1)
- Wilderness Medicine 11.20.2018Document12 pagesWilderness Medicine 11.20.2018Emily EresumaNo ratings yet
- Jaundice 11.28.2018Document13 pagesJaundice 11.28.2018Emily EresumaNo ratings yet
- Foster Care in Utah: Marlayna DespresDocument11 pagesFoster Care in Utah: Marlayna DespresEmily EresumaNo ratings yet
- Stem Cell Therapy For Rotator Cuff InjuriesDocument12 pagesStem Cell Therapy For Rotator Cuff InjuriesAthenaeum Scientific PublishersNo ratings yet
- GR Corplus Manual PDFDocument346 pagesGR Corplus Manual PDFAni Maulidia0% (1)
- Endoscopy Decontamination Policy: Name Title Institution Date Signature Written byDocument24 pagesEndoscopy Decontamination Policy: Name Title Institution Date Signature Written byJawad A. Al-LawatiNo ratings yet
- Library Genesis search for Stephen KochDocument7 pagesLibrary Genesis search for Stephen Kochyagogierlini2167No ratings yet
- NCM 109 Reviewer Module 1Document6 pagesNCM 109 Reviewer Module 1tamsmadjad18No ratings yet
- 1.1 Role of Organic Drug Molecules Unit 1Document16 pages1.1 Role of Organic Drug Molecules Unit 1Amarnath SahNo ratings yet
- A Case of Hodgkin Lymphoma Presenting As Nephrotic SyndromeDocument6 pagesA Case of Hodgkin Lymphoma Presenting As Nephrotic SyndromeIJAR JOURNALNo ratings yet
- Classroom Set-Up Food Vaccine FrequencyDocument5 pagesClassroom Set-Up Food Vaccine FrequencyLuke Edward PanganibanNo ratings yet
- Diabetic Retinopathy Treatment in MumbaiDocument7 pagesDiabetic Retinopathy Treatment in MumbaiCharvi JainNo ratings yet
- Infection Prevention and Control ProgramsDocument2 pagesInfection Prevention and Control ProgramsAnonymous HSZMNq4100% (1)
- Summary PsilocybinDocument1 pageSummary PsilocybintetaNo ratings yet
- Teaching Project Summary PaperDocument11 pagesTeaching Project Summary Paperapi-630699625No ratings yet
- Pharmacology Exam COHORT 8Document9 pagesPharmacology Exam COHORT 8Lesley Liavoga SandeNo ratings yet
- YAWAADocument10 pagesYAWAAZyrene CapulongNo ratings yet
- Nle ReviewerdianemaydeeDocument170 pagesNle ReviewerdianemaydeeSucceed ReviewNo ratings yet
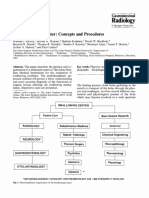
- 4.3 Swallowing - Center - Concepts - and - ProceduresDocument7 pages4.3 Swallowing - Center - Concepts - and - Proceduresluribe662No ratings yet
- Anaesthetic Case StudyDocument11 pagesAnaesthetic Case StudysomyntNo ratings yet
- CHAPTER 1 Thesis ProposalDocument2 pagesCHAPTER 1 Thesis ProposalPaul BejarNo ratings yet
- EndometritisDocument6 pagesEndometritisandriansyah2110% (1)
- Medical Specialty Recruitment Applicant Handbook 2021 v1.1Document50 pagesMedical Specialty Recruitment Applicant Handbook 2021 v1.1SamNo ratings yet
- Updated Workflow For Declaration of SGH Healthcare Workers With Covid-19 ExposureDocument6 pagesUpdated Workflow For Declaration of SGH Healthcare Workers With Covid-19 ExposureHazwan HafizuddinNo ratings yet
- RS PaperDocument12 pagesRS PaperGRAZ SHIEL HARINo ratings yet
- Research Proposal PresentationDocument19 pagesResearch Proposal Presentationapi-542965039No ratings yet
- Management of Minor Ailments by Community Pharmacists in Cebu, Philippines - An Exploratory StudyDocument8 pagesManagement of Minor Ailments by Community Pharmacists in Cebu, Philippines - An Exploratory StudyYancey AmboyNo ratings yet