You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Case Study AllDocument22 pagesCase Study AllGeraldine Gallaron - CasipongNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- MUST To KNOW in HematologyDocument46 pagesMUST To KNOW in HematologyRona Salando100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Bone Marrow Biopsy Interpretive GuidelinesDocument19 pagesBone Marrow Biopsy Interpretive Guidelinesdtoxic1No ratings yet
- LymphaticDocument111 pagesLymphaticJohn Eldenver AlmirolNo ratings yet
- Cadcam0213 PDFDocument52 pagesCadcam0213 PDFclaudia360No ratings yet
- Mid Year Test Paper 2012 Maths Year 3Document8 pagesMid Year Test Paper 2012 Maths Year 3shansugunaNo ratings yet
- Lymphomas and LeukemiasDocument27 pagesLymphomas and LeukemiasgraceNo ratings yet
- Robbins Pathology Chapter 13 - White Blood CellsDocument7 pagesRobbins Pathology Chapter 13 - White Blood Cellsscorpiosphinx7980% (5)
- Bone Marrow Morphology: Normal and Abnormal FindingsDocument51 pagesBone Marrow Morphology: Normal and Abnormal FindingsMohammed FareedNo ratings yet
- Sop HoshasDocument97 pagesSop Hoshasshansuguna100% (1)
- Sop HoshasDocument97 pagesSop Hoshasshansuguna100% (1)
- SynopsisDocument25 pagesSynopsisamankauratwal100% (1)
- SJK Tamil Ldg Riverside Champion DineshDocument1 pageSJK Tamil Ldg Riverside Champion DineshshansugunaNo ratings yet
- SJK Tamil LDG Riverside: Mathanraj A/L HemanathanDocument1 pageSJK Tamil LDG Riverside: Mathanraj A/L HemanathanshansugunaNo ratings yet
- Nelson MandelaDocument1 pageNelson MandelashansugunaNo ratings yet
- I THINK MapsDocument8 pagesI THINK MapsshansugunaNo ratings yet
- Roshan BodyDocument4 pagesRoshan BodyshansugunaNo ratings yet
- Exam BT 1 Year 5Document14 pagesExam BT 1 Year 5shansugunaNo ratings yet
- GPK Pentadbiran Sugunadevi A/P VeeranDocument2 pagesGPK Pentadbiran Sugunadevi A/P VeeranshansugunaNo ratings yet
- B. SemaiDocument24 pagesB. SemaishansugunaNo ratings yet
- B. Subjective Questions Answer All The Questions. A. Count and Write The Numbers in Numerals and WordsDocument4 pagesB. Subjective Questions Answer All The Questions. A. Count and Write The Numbers in Numerals and WordsshansugunaNo ratings yet
- MATH Yr1p1Document4 pagesMATH Yr1p1shansugunaNo ratings yet
- English Year 3 PDFDocument24 pagesEnglish Year 3 PDFIs East100% (1)
- To Perform Quality Certification On Complex Electro Mechanical EquipmentDocument2 pagesTo Perform Quality Certification On Complex Electro Mechanical EquipmentshansugunaNo ratings yet
- Hematology Oncology Consultants GuideDocument23 pagesHematology Oncology Consultants GuideJolaine ValloNo ratings yet
- Blood Film AbnormalitiesDocument26 pagesBlood Film AbnormalitiesSana Bushra100% (2)
- Blood Components: Red CellsDocument4 pagesBlood Components: Red Cellstan shin meiNo ratings yet
- Aplastic AnemiaDocument52 pagesAplastic AnemiaMARGARET BLANCHE NICOLASNo ratings yet
- Non-Hodgkin's LymphomasDocument23 pagesNon-Hodgkin's LymphomasshevmyrNo ratings yet
- Aplastic AnemiaDocument19 pagesAplastic AnemiaShara SampangNo ratings yet
- Hematologic DisordersDocument25 pagesHematologic DisordersDacillo GailleNo ratings yet
- Diagnosis of Multiple Myeloma From A Blood Sample Failed To Be Centrifuged A Case ReportDocument7 pagesDiagnosis of Multiple Myeloma From A Blood Sample Failed To Be Centrifuged A Case ReportHerbanu Haryo PramonoNo ratings yet
- Stem Cell - MD: The Ultimate Stroke Rehabilitation Program!Document4 pagesStem Cell - MD: The Ultimate Stroke Rehabilitation Program!David A. SteenblockNo ratings yet
- Class Participation VII in Cellular AberrationDocument2 pagesClass Participation VII in Cellular AberrationJacky SerquinaNo ratings yet
- Prabhu 2015Document5 pagesPrabhu 2015entannabilakasdyNo ratings yet
- Samar State University College of Nursing and Health SciencesDocument8 pagesSamar State University College of Nursing and Health SciencesThelda Mae Arteche SablanNo ratings yet
- The SkepasDocument24 pagesThe Skepasprince kumarNo ratings yet
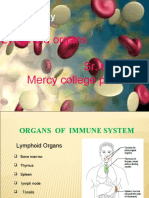
- Immunology: Lymphoid Organs Sr. Sarupya Mercy College PalakkadDocument28 pagesImmunology: Lymphoid Organs Sr. Sarupya Mercy College PalakkadTahir AzizNo ratings yet
- Understanding Acute Leukemia: Signs, Symptoms and TreatmentDocument46 pagesUnderstanding Acute Leukemia: Signs, Symptoms and TreatmentMaica LectanaNo ratings yet
- Hemopoiesis PDFDocument14 pagesHemopoiesis PDFrysnawahyu13No ratings yet
- Hema TransDocument10 pagesHema TransIya BangalanNo ratings yet
- Diagnosis of AnemiaDocument14 pagesDiagnosis of AnemiaAnggie AnggriyanaNo ratings yet
- AbbreviationsDocument239 pagesAbbreviationsMadras C RajasekarNo ratings yet
- Bone Marrow StudiesDocument3 pagesBone Marrow StudiesDELLNo ratings yet
- DE Bone Marrow VA30 syngoCTDocument2 pagesDE Bone Marrow VA30 syngoCTbajij57766No ratings yet