You might also like
- Gender and LaborDocument2 pagesGender and LaborCenon Paul SeronNo ratings yet
- Activity On Topic 1: Historical Antecedents in The Course of Science and TechnologyDocument2 pagesActivity On Topic 1: Historical Antecedents in The Course of Science and TechnologyRolly GabuyoNo ratings yet
- Unit 2-Topic 1-Physical SelfDocument9 pagesUnit 2-Topic 1-Physical SelfMab ShiNo ratings yet
- Rhythmic Gymnastics Exercise ProgramDocument28 pagesRhythmic Gymnastics Exercise Programlyra cosgafaNo ratings yet
- Indigenous Science PDFDocument10 pagesIndigenous Science PDFShane Naig RoganNo ratings yet
- Sample Narrative ReportDocument2 pagesSample Narrative ReportAnonymous GGZpZWNo ratings yet
- Alfredo v. LagmayDocument10 pagesAlfredo v. LagmayMakent John SantiagoNo ratings yet
- Title: The Political CartoonsDocument6 pagesTitle: The Political CartoonsShiela Marie GadayosNo ratings yet
- Activity Gene TherapyDocument3 pagesActivity Gene TherapyKent Gabriel YangaoNo ratings yet
- Kitchen Safety: Precautions and First Aid: Study Guide L Module No.5Document12 pagesKitchen Safety: Precautions and First Aid: Study Guide L Module No.5Marlyn MabalotNo ratings yet
- Genes and Their Role in Animal Productivity: Introduction To Animal ScienceDocument28 pagesGenes and Their Role in Animal Productivity: Introduction To Animal Sciencedreih MadrigNo ratings yet
- Science, Technology and Society (Module 2)Document16 pagesScience, Technology and Society (Module 2)Pixl MixNo ratings yet
- Bullying (Persuasive Essay Sample)Document3 pagesBullying (Persuasive Essay Sample)iamJairaAmoncio100% (1)
- Understanding The Self Lesson 1 4Document98 pagesUnderstanding The Self Lesson 1 4Christian DelacruzNo ratings yet
- Peuthenics Prefinals Task PerformanceDocument5 pagesPeuthenics Prefinals Task PerformanceGelo MoloNo ratings yet
- (UTS) Perspectives - PhilosophyDocument10 pages(UTS) Perspectives - PhilosophyAlyssa Crizel CalotesNo ratings yet
- Read The Article - Then, Answer The Question That FollowDocument1 pageRead The Article - Then, Answer The Question That FollowEldrick Neil ReyesNo ratings yet
- The Material and Formal Object of EthicsDocument22 pagesThe Material and Formal Object of EthicsDave SaldivarNo ratings yet
- Canadian Dining EtiquetteDocument7 pagesCanadian Dining EtiquetteAndarifaNo ratings yet
- Understanding History Through Primary and Secondary SourcesDocument40 pagesUnderstanding History Through Primary and Secondary SourcesNickhol Tantiongco0% (1)
- Psych 101 Lesson 5.1 The Physical and Sexual Self Part 1Document9 pagesPsych 101 Lesson 5.1 The Physical and Sexual Self Part 1Rigel LimaNo ratings yet
- Important PeopleDocument6 pagesImportant Peoplemicahkaye17No ratings yet
- Activity1.2.what Is Self - UTSDocument3 pagesActivity1.2.what Is Self - UTSJhon dave Surbano100% (1)
- El PresidenteDocument2 pagesEl PresidenteGuss IstwofeedNo ratings yet
- V. The Filipinization of Personality TheoryDocument28 pagesV. The Filipinization of Personality TheorylfhippocampusNo ratings yet
- Act 19 UTS TacmoyDocument3 pagesAct 19 UTS TacmoyEdrian TacmoyNo ratings yet
- Story of My LifeDocument1 pageStory of My LifePlong PlongNo ratings yet
- Lesson 1 Vision Mission Core Values Objectives of The InstitutionDocument2 pagesLesson 1 Vision Mission Core Values Objectives of The InstitutionKrixie LagundiNo ratings yet
- Types of Dances: ObjectivesDocument9 pagesTypes of Dances: ObjectivesjohnNo ratings yet
- GE8 - Lesson 1 - Moral and Non Moral Standards - Sy2022 23Document13 pagesGE8 - Lesson 1 - Moral and Non Moral Standards - Sy2022 23Mary Grace IlaganNo ratings yet
- Unit 7 THE SELF IN FACING CHALLENGESDocument12 pagesUnit 7 THE SELF IN FACING CHALLENGESJohn Lexter Sarmiento BoneoNo ratings yet
- STS Module 5Document4 pagesSTS Module 5Angel Justine BernardoNo ratings yet
- History Handout - Unedited Copy, Instructor'sDocument39 pagesHistory Handout - Unedited Copy, Instructor'sleapapayNo ratings yet
- Paulo C. Campos: (July 7, 1921 - June 2, 2007)Document3 pagesPaulo C. Campos: (July 7, 1921 - June 2, 2007)NanceNo ratings yet
- Read Phil HisDocument8 pagesRead Phil HisMichNo ratings yet
- RISK MANAGEMENT APPLIED TO FOOD SAFETY FLOWDocument3 pagesRISK MANAGEMENT APPLIED TO FOOD SAFETY FLOWLea Mae100% (1)
- Reflection on "Oooppss, Kumukulo ang tiyan ni JimboDocument1 pageReflection on "Oooppss, Kumukulo ang tiyan ni JimboDaniel ZuniegaNo ratings yet
- 1Document1 page1arizaldo0% (2)
- Social Influence, Conformity and Moral DevelopmentDocument30 pagesSocial Influence, Conformity and Moral DevelopmentJay GrijaldoNo ratings yet
- PE NotesDocument20 pagesPE NotesAlma C WalshNo ratings yet
- Agri 111Document2 pagesAgri 111She LlaNo ratings yet
- Recreation: Pass CollegeDocument3 pagesRecreation: Pass CollegeMary Ann F. Mendez0% (1)
- Chapter 3 - Drug EducationDocument26 pagesChapter 3 - Drug EducationHabadu HabadiNo ratings yet
- The Health Benefits of Playing BasketballDocument1 pageThe Health Benefits of Playing BasketballMark Luigie CalanogNo ratings yet
- Different Division of ZoologyDocument2 pagesDifferent Division of ZoologyEiann Jasper LongcayanaNo ratings yet
- Chapter II RRLDocument11 pagesChapter II RRLFrances50% (2)
- AEC16 Strategies To Effect AdoptionDocument12 pagesAEC16 Strategies To Effect AdoptionVanshence neosilverNo ratings yet
- 12 Annoying Attitudes of Filipinos We Need To Get Rid Of"Document13 pages12 Annoying Attitudes of Filipinos We Need To Get Rid Of"Renato LorillaNo ratings yet
- Sigmund Freud EssayDocument8 pagesSigmund Freud EssayFor Valor100% (1)
- Unit 1.a - Beginnings of Sikolohiyang PilipinoDocument5 pagesUnit 1.a - Beginnings of Sikolohiyang PilipinoJoan FranciscoNo ratings yet
- MST Lesson 6 - Soil and Land ResourcesDocument39 pagesMST Lesson 6 - Soil and Land ResourcesPolNo ratings yet
- Dissection of A House Lizard PDFDocument3 pagesDissection of A House Lizard PDFJustin KyleNo ratings yet
- Golden Rice falls short on lifesaving promisesDocument6 pagesGolden Rice falls short on lifesaving promisesKen lopezNo ratings yet
- Ethical JudgmentDocument13 pagesEthical JudgmentprimokelzNo ratings yet
- GE STS Notes For PrelimDocument5 pagesGE STS Notes For PrelimLyle Abe Fuego Dampog100% (1)
- STS 10 Ch.1 Lesson 2 - Science, Technology and National DevelopmentDocument2 pagesSTS 10 Ch.1 Lesson 2 - Science, Technology and National DevelopmentVanessa Enanoria AsaiasNo ratings yet
- PineappleDocument18 pagesPineappleJomairah BangcolaNo ratings yet
- Module On Gecsel: Understanding The SelfDocument42 pagesModule On Gecsel: Understanding The SelfJpoy RiveraNo ratings yet
- Pests of Field Crops and Pastures: Identification and ControlFrom EverandPests of Field Crops and Pastures: Identification and ControlNo ratings yet
- D Factors Influencing MH PlainDocument11 pagesD Factors Influencing MH PlainConrad C. CatimbangNo ratings yet
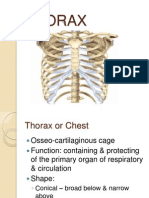
- ThoraxDocument20 pagesThoraxmr_davidNo ratings yet
- Usmle Step 1 CrosswordsDocument210 pagesUsmle Step 1 Crosswordsmr_david50% (2)
- Usmle Free 150Document44 pagesUsmle Free 150ironslave100% (1)
- 10 Ways To Succeed With USMLE Step 1Document19 pages10 Ways To Succeed With USMLE Step 1Zunaira Abdul Ghaffar100% (2)
- 10 Ways To Succeed With USMLE Step 1Document19 pages10 Ways To Succeed With USMLE Step 1Zunaira Abdul Ghaffar100% (2)
- Doctor-Patient Relationship: Hyacinth C. Manood, MD, FPPADocument25 pagesDoctor-Patient Relationship: Hyacinth C. Manood, MD, FPPAmr_davidNo ratings yet
- Ophthalmology Notes Visual GuideDocument81 pagesOphthalmology Notes Visual Guidemr_david50% (2)
- PedsSamplex CardiologyDocument18 pagesPedsSamplex Cardiologymr_davidNo ratings yet
- Brain and BehaviorDocument16 pagesBrain and Behaviormr_davidNo ratings yet
- Shizophrenia Other Psychotic Disorders: Hyacinth C. Manood, MD, DPBPDocument56 pagesShizophrenia Other Psychotic Disorders: Hyacinth C. Manood, MD, DPBPDani NugrohoNo ratings yet
- Psychosis Due To Endocrine DISTURBANCESDocument47 pagesPsychosis Due To Endocrine DISTURBANCESmr_davidNo ratings yet
- Brain & Human BehaviourDocument45 pagesBrain & Human Behaviourmr_davidNo ratings yet
- Lacan - Case of AimeeDocument8 pagesLacan - Case of AimeeCyril SuNo ratings yet
- Who Is DiagnosableDocument3 pagesWho Is DiagnosableHamna Shahid100% (1)
- SCHIZOPHRENIADocument5 pagesSCHIZOPHRENIAsri nandiniNo ratings yet
- PSY 3410 Autism Spectrum Disorders & Intellectual DisabilityDocument26 pagesPSY 3410 Autism Spectrum Disorders & Intellectual Disabilityncastro1319No ratings yet
- Nursing Care Plan Autism Spectrum DisorderDocument1 pageNursing Care Plan Autism Spectrum DisorderHarold Peranduz100% (5)
- Psych Abnormal Child Psychology - 6th Edition (2015) - 601-658Document58 pagesPsych Abnormal Child Psychology - 6th Edition (2015) - 601-658tin_ally9059No ratings yet
- Draft Part 1. Choose The Best Single Answer (BSA) by Encircling Its Corresponding LetterDocument11 pagesDraft Part 1. Choose The Best Single Answer (BSA) by Encircling Its Corresponding LetterKhadar mohamedNo ratings yet
- Therapy PDFDocument186 pagesTherapy PDFRuMarlop MartinezNo ratings yet
- Cardo & Barceló (2005) PDFDocument5 pagesCardo & Barceló (2005) PDFAna Catarina InácioNo ratings yet
- Psychia ExamDocument19 pagesPsychia ExamEdz Votefornoymar Del RosarioNo ratings yet
- 2somatoformquiz SNDocument2 pages2somatoformquiz SNmalindaNo ratings yet
- How-To-Cope-With-Hearing-Voices 2016Document22 pagesHow-To-Cope-With-Hearing-Voices 2016api-247002951No ratings yet
- Autism Spectrum Disorder (ASD) in Girls. Co-Occurring Psychopathology. Sex Differences in Clinical ManifestationDocument11 pagesAutism Spectrum Disorder (ASD) in Girls. Co-Occurring Psychopathology. Sex Differences in Clinical ManifestationRania shafiraNo ratings yet
- ManiaDocument10 pagesManiaaashvi dalalNo ratings yet
- CatatoniaDocument40 pagesCatatoniaRicha PariharNo ratings yet
- SCHIZOAFFECTIVEDocument37 pagesSCHIZOAFFECTIVEDhea Faizia TasyaNo ratings yet
- Mental Status Exam FindingsDocument4 pagesMental Status Exam Findingsjoshua canjaNo ratings yet
- A List of Psychological DisordersDocument12 pagesA List of Psychological DisordersGaurav LahotiNo ratings yet
- Psychosurgery: Year 11 GCSE Psychology Key Topic 8: AggressionDocument2 pagesPsychosurgery: Year 11 GCSE Psychology Key Topic 8: AggressionFaisal AhmedNo ratings yet
- I. General ObjectiveDocument5 pagesI. General ObjectiveMr. BQNo ratings yet
- Assessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.ArchanaaDocument62 pagesAssessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.Archanaadrkadiyala267% (3)
- Argumentative EssayDocument5 pagesArgumentative Essayapi-388945643No ratings yet
- Postpartum DepressionDocument28 pagesPostpartum DepressionRiza Angela Barazan100% (1)
- Thérapies Comportementales Et Cognitives Centrées Sur Les Schémas de Young Dans Les Troubles de La Personnalité: Étude Pilote Sur 14 CasDocument7 pagesThérapies Comportementales Et Cognitives Centrées Sur Les Schémas de Young Dans Les Troubles de La Personnalité: Étude Pilote Sur 14 CasJosephine Al FrangiNo ratings yet
- Initial Consult Note TemplateDocument2 pagesInitial Consult Note TemplateAmanda Caroline Bowers100% (1)
- 0674046498Document288 pages0674046498perac100% (4)
- TBH & TDAH Comorbidity of Attention Deficit Hyperactivity Disorder With Early - and Late-Onset BipDocument3 pagesTBH & TDAH Comorbidity of Attention Deficit Hyperactivity Disorder With Early - and Late-Onset BipVeio MacieiraNo ratings yet
- 1.51.1 (PSYCH) Psychiatric Disorders and AddictionDocument3 pages1.51.1 (PSYCH) Psychiatric Disorders and AddictionAndriel Gayle P. YuloNo ratings yet
- Jonathan S. Abramowitz - Understanding and Treating Obsessive-Compulsive Disorder. A Cognitive Behavioral Approach (2005)Document409 pagesJonathan S. Abramowitz - Understanding and Treating Obsessive-Compulsive Disorder. A Cognitive Behavioral Approach (2005)Ángela María Páez Buitrago100% (1)
- Three Categories of AutismDocument14 pagesThree Categories of Autismapi-327260204No ratings yet