You might also like
- Liver Function Test FinalDocument98 pagesLiver Function Test FinalHussain AzharNo ratings yet
- Congenital SyphilisDocument6 pagesCongenital SyphilisFrozen Pandora MahayaNo ratings yet
- Physical Growth and Development: Different Aspects and AssessmentDocument60 pagesPhysical Growth and Development: Different Aspects and AssessmentDipti RamiNo ratings yet
- Hematology & Immune SystemDocument81 pagesHematology & Immune SystemAmanuel Maru100% (1)
- Foetal CirculationDocument8 pagesFoetal CirculationMujahid_Dean_8976No ratings yet
- MeningitisDocument12 pagesMeningitisFaith Vaughn100% (2)
- Idiopathic Thrombocytopenic PurpuraDocument10 pagesIdiopathic Thrombocytopenic PurpuramariakolandaNo ratings yet
- Emergency Care (Hemophilia)Document30 pagesEmergency Care (Hemophilia)Nica Georgelle Maniego SamonteNo ratings yet
- Neonatal Exchange Transfusion GuideDocument9 pagesNeonatal Exchange Transfusion GuidedewpraNo ratings yet
- 5 FMCH Research BiasDocument3 pages5 FMCH Research BiasMia CadizNo ratings yet
- Health Assessment MCQs QuizDocument6 pagesHealth Assessment MCQs QuizAddisu Sertsu100% (1)
- Diabetes NotesDocument10 pagesDiabetes Notestripj33No ratings yet
- VDRL Test and Its InterpretationDocument11 pagesVDRL Test and Its InterpretationSauZen SalaZarNo ratings yet
- Unit VII Assessment of The Pediatric ClientDocument36 pagesUnit VII Assessment of The Pediatric ClientSyed Maaz100% (1)
- Imnci PPT KapilDocument65 pagesImnci PPT KapilkapilNo ratings yet
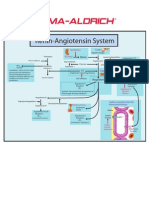
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Celiac Disease in ChildrenDocument59 pagesCeliac Disease in Childrend-fbuser-57045067No ratings yet
- Anaemia in Pregnancy: By-Dr. Soumya.p (2nd Yr PG) Mod - Dr. Rita. D (Professor and Hod)Document98 pagesAnaemia in Pregnancy: By-Dr. Soumya.p (2nd Yr PG) Mod - Dr. Rita. D (Professor and Hod)SoumyaNo ratings yet
- Transplantation: Presented by Santhiya K II M.SC Biotechnology 18PBT014Document54 pagesTransplantation: Presented by Santhiya K II M.SC Biotechnology 18PBT014AbiNo ratings yet
- ANATOMY and PHYSIOLOGY of CHRONIC OTITIS MEDIA-GCS Sa MED - ANNEX-maam ValezaDocument36 pagesANATOMY and PHYSIOLOGY of CHRONIC OTITIS MEDIA-GCS Sa MED - ANNEX-maam ValezaBonieve Pitogo NoblezadaNo ratings yet
- Etat + PDFDocument56 pagesEtat + PDFShandy BNo ratings yet
- Reproductive System Male and FemaleDocument61 pagesReproductive System Male and FemaleAsad KHAN100% (1)
- Chapter 14 - HematopathologyDocument66 pagesChapter 14 - Hematopathologynigel farageNo ratings yet
- Lecture Hemophilia and Thrombocytopenic PurpuraDocument55 pagesLecture Hemophilia and Thrombocytopenic PurpuraaymenNo ratings yet
- Introduction of Medical Surgical NursingDocument86 pagesIntroduction of Medical Surgical NursingSeema YadavNo ratings yet
- ABO Incompatibility in NeonateDocument27 pagesABO Incompatibility in NeonatemarshalitaNo ratings yet
- RH IcompatibilityDocument3 pagesRH IcompatibilitySourabh SharafNo ratings yet
- LeukocoriaDocument29 pagesLeukocoriaDevi Ariani100% (1)
- Idiopathic Thrombocytopenic Purpura Case StudyDocument38 pagesIdiopathic Thrombocytopenic Purpura Case StudyKurbulNo ratings yet
- Blood Transfusion FinalDocument8 pagesBlood Transfusion FinalejkohNo ratings yet
- CM Gastric and Duodenal Contents Examination (Ocfemia, Eliazel G - BSMT4-PLTCI)Document53 pagesCM Gastric and Duodenal Contents Examination (Ocfemia, Eliazel G - BSMT4-PLTCI)eliazel ocfemiaNo ratings yet
- SummaryDocument4 pagesSummaryDyam MitchNo ratings yet
- Leukemia (Partly)Document9 pagesLeukemia (Partly)rukipatNo ratings yet
- Beta ThalassaemiaDocument10 pagesBeta ThalassaemiaJoyce TeoNo ratings yet
- Medical Diseases Complicating Pregnancy: by The Name of AllahDocument45 pagesMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيNo ratings yet
- Pathology - Abnormal Cell Growth PDFDocument28 pagesPathology - Abnormal Cell Growth PDFAmirul ZackNo ratings yet
- Ectopic PregnancyDocument76 pagesEctopic PregnancyVivian Jean TapayaNo ratings yet
- (Pelvic Inflammatory Disease) Samiya AhmedDocument31 pages(Pelvic Inflammatory Disease) Samiya AhmedSaamiya AhmedNo ratings yet
- Manual 24 Hour RecallDocument160 pagesManual 24 Hour RecallMadalina CervidNo ratings yet
- Hepatitis GDocument8 pagesHepatitis Ghelmi0% (1)
- Medscape Status EpilepticusDocument10 pagesMedscape Status EpilepticusEllen Siska SusantiNo ratings yet
- ITP (Idiopathic Thrombocytopenic Purpura)Document20 pagesITP (Idiopathic Thrombocytopenic Purpura)Iqra NaseemNo ratings yet
- Submitted By: Diana M. Resultay A301/Group-3B Submitted To: Ms. ReyesDocument9 pagesSubmitted By: Diana M. Resultay A301/Group-3B Submitted To: Ms. ReyesDiannetotz MoralesNo ratings yet
- Hepatitis ADocument1 pageHepatitis AGary Detman100% (1)
- Nephrotic SyndromeeDocument28 pagesNephrotic SyndromeeRiteka SinghNo ratings yet
- CBC InterpretationDocument6 pagesCBC InterpretationKate Basa100% (1)
- Neonatal SepsisDocument17 pagesNeonatal SepsisDhilla Feroh Kesuma TNo ratings yet
- Endang Windiastuti Division of Hematology-Oncology Department of Child Health DR Cipto Mangunkusumo Hospital, FMUIDocument27 pagesEndang Windiastuti Division of Hematology-Oncology Department of Child Health DR Cipto Mangunkusumo Hospital, FMUIAnonymous NRDU0bLFSNo ratings yet
- Von Willebrand DiseaseDocument9 pagesVon Willebrand DiseaserandyNo ratings yet
- Hemolytic Disease of The NewbornDocument43 pagesHemolytic Disease of The Newbornalibayaty1No ratings yet
- ABO IncompatibilityDocument2 pagesABO IncompatibilityeirikaesatcioNo ratings yet
- Transfusion of Blood & Blood Components1Document45 pagesTransfusion of Blood & Blood Components1Chamika Huruggamuwa100% (1)
- 2018 Overview Digestive System HandoutDocument11 pages2018 Overview Digestive System HandoutdraganNo ratings yet
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Tietz's Applied Laboratory MedicineFrom EverandTietz's Applied Laboratory MedicineMitchell G. ScottRating: 3 out of 5 stars3/5 (1)
- Practical Gastroenterology and Hepatology Board Review ToolkitFrom EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultNo ratings yet
- A Review of Breast Cancer Research in Malaysia: CH Yip, FRCS, N Bhoo Pathy, MD, SH Teo, PHDDocument15 pagesA Review of Breast Cancer Research in Malaysia: CH Yip, FRCS, N Bhoo Pathy, MD, SH Teo, PHDRoshandiep GillNo ratings yet
- Pharmpract 08 029Document6 pagesPharmpract 08 029Roshandiep GillNo ratings yet
- APJCP - Volume 11 - Issue 6 - Pages 1503-1508Document6 pagesAPJCP - Volume 11 - Issue 6 - Pages 1503-1508Roshandiep GillNo ratings yet
- S6-Ankle Ligament InjuryDocument17 pagesS6-Ankle Ligament InjuryRoshandiep GillNo ratings yet
- Pediatric Medical History FormDocument2 pagesPediatric Medical History FormRoshandiep Gill100% (1)
- Long Cases ABM ABDULLAH 1st Edition PDFDocument844 pagesLong Cases ABM ABDULLAH 1st Edition PDFProthoma Dey64% (11)
- Pediatrics History TakingDocument2 pagesPediatrics History TakingRoshandiep GillNo ratings yet
- Case Write Up Obstetrics Gestational Diabetes MellitusDocument13 pagesCase Write Up Obstetrics Gestational Diabetes MellitusRoshandiep GillNo ratings yet
- Erb's Palsy SeminarDocument10 pagesErb's Palsy SeminarRoshandiep GillNo ratings yet
- Anaesthesia For Medical StudentDocument266 pagesAnaesthesia For Medical Studentprevet100% (4)
- Guidelines for Inpatient Pharmacy PracticeDocument68 pagesGuidelines for Inpatient Pharmacy PracticeAmir Ihsan100% (1)
- Dengue Fever 4Document65 pagesDengue Fever 4Roshandiep GillNo ratings yet
- Pre-Malignant Conditions Screening Modalitiespptx PDFDocument39 pagesPre-Malignant Conditions Screening Modalitiespptx PDFRoshandiep GillNo ratings yet
- Acne Vulgaris and Rosacea Treatment GuideDocument33 pagesAcne Vulgaris and Rosacea Treatment GuideRoshandiep GillNo ratings yet
- Radial Nerve Palsy: - Aetiology, Clinical FeaturesDocument9 pagesRadial Nerve Palsy: - Aetiology, Clinical FeaturesRoshandiep GillNo ratings yet
- Hwee S O G A4 Spiral PDFDocument143 pagesHwee S O G A4 Spiral PDFeric sivaneshNo ratings yet
- Pediatrics History TakingDocument2 pagesPediatrics History TakingRoshandiep GillNo ratings yet
- QUESTION 85 ObgynDocument1 pageQUESTION 85 ObgynRoshandiep GillNo ratings yet
- Knee Injury: By: Haspreet GillDocument18 pagesKnee Injury: By: Haspreet GillRoshandiep GillNo ratings yet
- WilsonDocument8 pagesWilsonRoshandiep GillNo ratings yet
- Head and Neck TraumaDocument24 pagesHead and Neck TraumaRoshandiep GillNo ratings yet
- Treatment of SorethroatDocument2 pagesTreatment of SorethroatRoshandiep GillNo ratings yet
- Seminar Obgyn Chemotheraphy in GynaecologyDocument38 pagesSeminar Obgyn Chemotheraphy in GynaecologyRoshandiep GillNo ratings yet
- Malaysia Normal Pregnant Care PDFDocument251 pagesMalaysia Normal Pregnant Care PDFHavenesh Rao100% (2)
- Multiple Myeloma: By: Haspreet Kaur GillDocument19 pagesMultiple Myeloma: By: Haspreet Kaur GillRoshandiep GillNo ratings yet
- A Review of Breast Cancer Research in Malaysia: CH Yip, FRCS, N Bhoo Pathy, MD, SH Teo, PHDDocument15 pagesA Review of Breast Cancer Research in Malaysia: CH Yip, FRCS, N Bhoo Pathy, MD, SH Teo, PHDRoshandiep GillNo ratings yet
- Journal Obgyn PDFDocument16 pagesJournal Obgyn PDFRoshandiep GillNo ratings yet
- Family Medicine Skin LesionsDocument3 pagesFamily Medicine Skin LesionsRoshandiep GillNo ratings yet
- Scan 20200625Document1 pageScan 20200625Roshandiep GillNo ratings yet
- LMH New Patient PacketDocument10 pagesLMH New Patient PackettytrytrNo ratings yet
- Running Faster Than NyquistDocument6 pagesRunning Faster Than NyquistHossain Mohammad MahbubNo ratings yet
- User Manual of VT310Document15 pagesUser Manual of VT310Yiditechcorp SANo ratings yet
- Strategic Planning Ebook 2021 HRDocument8 pagesStrategic Planning Ebook 2021 HRJosé F. NetoNo ratings yet
- CPT-720 Portable Terminal Power and Environmental SpecsDocument2 pagesCPT-720 Portable Terminal Power and Environmental SpecsSantoso LeonardiNo ratings yet
- Meals in The UKDocument5 pagesMeals in The UKAna Monica Conrado PereaNo ratings yet
- Answer Sheet Grade 12 Online/BlendedDocument3 pagesAnswer Sheet Grade 12 Online/BlendedMark Earvin CervantesNo ratings yet
- Assessment Form 10 (Collection and Analysis of Quantitative and Qualitative Data) 3Document8 pagesAssessment Form 10 (Collection and Analysis of Quantitative and Qualitative Data) 3Raymond RamirezNo ratings yet
- Fabb Nigel CompoundingDocument18 pagesFabb Nigel CompoundingMüge AkcanNo ratings yet
- Subject: Biochemistry Topic:Lipid Metabolism 2 Lecturer: Dr. Laygo DATE: NOV. 2010Document11 pagesSubject: Biochemistry Topic:Lipid Metabolism 2 Lecturer: Dr. Laygo DATE: NOV. 2010Std DlshsiNo ratings yet
- Nature's Serenity and Artistic InspirationDocument2 pagesNature's Serenity and Artistic InspirationGuilherme Daniel ColtreNo ratings yet
- Case Studies On Threats To Audit IndependenceDocument3 pagesCase Studies On Threats To Audit IndependencedemolaojaomoNo ratings yet
- Catalogue For TeethDocument47 pagesCatalogue For TeethaleruhoNo ratings yet
- Franchising Pancake House in Tacloban CityDocument35 pagesFranchising Pancake House in Tacloban CityHell Yeah100% (1)
- Enhancing Passenger Experience at Heathrow AirportDocument23 pagesEnhancing Passenger Experience at Heathrow AirportDhruvi JhaveriNo ratings yet
- Finding the intersection point of two linesDocument10 pagesFinding the intersection point of two linesLinh LêNo ratings yet
- Ipd Workflow FinalDocument1 pageIpd Workflow Finalapi-31765881No ratings yet
- ASIAN INSTITUTE OF TECHNOLOGY WORK IMMERSION AT RYONAN ELECTRICDocument18 pagesASIAN INSTITUTE OF TECHNOLOGY WORK IMMERSION AT RYONAN ELECTRICAngelo DonesNo ratings yet
- HDocument6 pagesHJohn ManciaNo ratings yet
- Institutional Support For New VenturesDocument8 pagesInstitutional Support For New VenturesAdeem AshrafiNo ratings yet
- 6apr21 Emergency Motion Supreme Court of VirginiaDocument4 pages6apr21 Emergency Motion Supreme Court of VirginiaJaniceWolkGrenadierNo ratings yet
- FIITJEE AITS PAPER2 MDocument23 pagesFIITJEE AITS PAPER2 MshreyashNo ratings yet
- Origin Destination Flight No. Aircraft Days of Departure Arrival Type Operation Time TimeDocument38 pagesOrigin Destination Flight No. Aircraft Days of Departure Arrival Type Operation Time Timekulkarni68No ratings yet
- Replacement of Metallic Automobile Components with Polymer CompositesDocument3 pagesReplacement of Metallic Automobile Components with Polymer CompositesKris EdoNo ratings yet
- Update National Sales Conference - RUNDOWN 21april2021Document1 pageUpdate National Sales Conference - RUNDOWN 21april2021NasrudinNo ratings yet
- Hero Journey UnitDocument4 pagesHero Journey Unitgaby yepesNo ratings yet
- Zakynthos - Greece enDocument32 pagesZakynthos - Greece ensilversurfer3100% (4)
- Research Paper Worksheet Middle SchoolDocument5 pagesResearch Paper Worksheet Middle Schoolorotmbbkf100% (1)
- MArketing Research Notes Chapter 20Document14 pagesMArketing Research Notes Chapter 20manojpatel51100% (1)
- Filters for Hydraulic ExcavatorsDocument18 pagesFilters for Hydraulic ExcavatorsTan JaiNo ratings yet
- DID 180 Standard Roller Chain: Roller Chains For Power TransmissionDocument1 pageDID 180 Standard Roller Chain: Roller Chains For Power TransmissionJhampol Rosales MuñozNo ratings yet