You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DR Wong Teck WeeipadDocument2 pagesDR Wong Teck Weeipadtwwong68No ratings yet
- Hyperthermia and Risk For AspirationDocument3 pagesHyperthermia and Risk For AspirationAlmyr RimandoNo ratings yet
- ADS ADEA ANZCA NZSSD - DKA - SGLT2i - Alert - Ver July 2022Document3 pagesADS ADEA ANZCA NZSSD - DKA - SGLT2i - Alert - Ver July 2022tom.condon.02No ratings yet
- HSPK 2021Document270 pagesHSPK 2021Sabrina Agustien SimanungkalitNo ratings yet
- Academica Science Journal PSYCHOLOGICA - No 2Document3 pagesAcademica Science Journal PSYCHOLOGICA - No 2Ciotea ValentinNo ratings yet
- Kriya For Balancing The ChakrasDocument5 pagesKriya For Balancing The ChakrasFedra Fox Cubeddu100% (2)
- Cephalometric Evaluation and Measurement of The Upper Airway PDFDocument13 pagesCephalometric Evaluation and Measurement of The Upper Airway PDFSoe San KyawNo ratings yet
- Vol 19.1 - Sleep Disorders.2013Document252 pagesVol 19.1 - Sleep Disorders.2013Martoiu MariaNo ratings yet
- CV DermatologistDocument2 pagesCV DermatologistArys SetiawanNo ratings yet
- YamamotoDocument11 pagesYamamotolopezhectora100% (1)
- ReviewerDocument20 pagesReviewerYang MolosNo ratings yet
- The JFK AutopsyDocument6 pagesThe JFK AutopsysithusoemoeNo ratings yet
- Introduction to Radiographic Imaging InterpretationDocument17 pagesIntroduction to Radiographic Imaging Interpretationpradep4u21No ratings yet
- LMA Fast TrackDocument2 pagesLMA Fast TrackLeandro AlmeidaNo ratings yet
- Makalah Bahasa InggrisDocument2 pagesMakalah Bahasa InggrisOlga RevalinaNo ratings yet
- List of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Document5 pagesList of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Sunira EnterprisesNo ratings yet
- HIMSS EMRAM Stage 7 DMTDocument20 pagesHIMSS EMRAM Stage 7 DMTclrhoadesNo ratings yet
- References Style and Writing GuideDocument23 pagesReferences Style and Writing GuideHarshal SabaneNo ratings yet
- HypothyroidismfinalpptDocument91 pagesHypothyroidismfinalpptswathi bsNo ratings yet
- Features FNCP:: Health Nursing ProblemsDocument12 pagesFeatures FNCP:: Health Nursing Problemsrodeliza100% (2)
- Influence of Cavity LiningDocument7 pagesInfluence of Cavity Liningpatel keralNo ratings yet
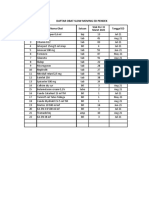
- Daftar Obat Slow Moving Dan Ed Rawat Inap Maret 2021Document8 pagesDaftar Obat Slow Moving Dan Ed Rawat Inap Maret 2021Vima LadipaNo ratings yet
- Calcaneum Fractures: Jensen Joseph GMC KannurDocument104 pagesCalcaneum Fractures: Jensen Joseph GMC KannurAmel VnairNo ratings yet
- RAV Admission Notice for Ayurveda CoursesDocument4 pagesRAV Admission Notice for Ayurveda CoursesBhargav KalalNo ratings yet
- YOU IN SURGICAL - Product CatalogDocument222 pagesYOU IN SURGICAL - Product CatalogfarazNo ratings yet
- EFN - PPTX 3Document9 pagesEFN - PPTX 3Suheni Khotimah IndrianiNo ratings yet
- Akupuntur 7Document9 pagesAkupuntur 7Ratrika SariNo ratings yet
- Science 5Document81 pagesScience 5Michael Joseph Santos100% (2)
- Clinical Experience With The Constellation Vision SystemDocument16 pagesClinical Experience With The Constellation Vision SystemMohammad Abdullah BawtagNo ratings yet